Understanding Vaccine Hesitancy Amongst Frontline Workers
The influence of trade union and community representatives
By Sian Moore, Calvin Burns, Nigel Carter, Christina Clamp, Wesley Martin and Eklou Amendah
Download PDF report
- Published by
- The British Academy
- Year
- 2022
- Pages
- 31
About the authors
Professor Sian Moore is Professor in Employment Relations and Human Resource Management at the Centre for Research on Employment and Work at the University of Greenwich. Professor Christina Clamp is Professor of Sociology at the Center for Co-operatives & CED at the Southern New Hampshire University. Eklou R Amendah is Assistant Professor of Marketing at the University of Southern Maine. Dr Nigel Carter is a Research Fellow at the Centre for Research on Employment and Work at the University of Greenwich. Dr Calvin Burns is a Senior Lecturer in Occupational Psychology in the School of Human Sciences at the University of Greenwich. Wesley Martin is a Research Assistant at the Southern New Hampshire University.
Acknowledgements
The authors would like to thank the British Academy for their support for this study, particularly the assistance of Flora Langley. Above all they extend gratitude to all those who spared time to be interviewed or participated in focus groups as part of the research.
About the COVID-19 Recovery: Building Future Pandemic Preparedness and Understanding Citizen Engagement in the USA and UK
The programme is the result of a partnership between the British Academy, the Social Sciences Research Council (SSRC) and the Science & Innovation Network in the USA (SIN USA) to award funding to 10 transatlantic studies focusing on UK-US COVID-19 vaccine engagement. It follows a pilot study exploring levels of vaccine engagement in four locations across the US and UK, while the larger programme was expanded to study multiple locations. The programme was funded by the UK’s Department for Business, Energy and Industrial Strategy.
Introduction
This study explores how longstanding structural inequalities that informed experiences of working through COVID-19 manifest in the decisions frontline workers make about vaccination. There is a focus on BME/BIPOC(1) workers because of their predominance among frontline workers during the pandemic and thus disproportionate vulnerability to COVID-19. However, in its concentration on work, the study hopes to address the dangers of racializing vaccination. It locates workers and workplaces in their wider communities and explores the interaction of work and community influences. A US-UK comparison allows for interrogation of contexts shaped by place, culture, social, political and economic factors. It permits comparison of health and welfare infrastructures and of culturally sensitive healthcare systems and how these shape worker responses to vaccines. The study examines the factors informing vaccine hesitancy (using the UK SAGE definition that ‘hesitancy refers to delay in acceptance or refusal of vaccines despite availability of vaccine services’) in the context of work and the workplace and organisational rules and expectations on vaccination. It explores the role of trade unions and community organisations in negotiating or mediating vaccination and in engaging workers and the community in vaccination programmes, while being sensitive to potential tensions. In the US this includes homeless communities, disproportionately people of color.
The COVID-19 literature can overlook work and occupational health and safety and the key role employers and trade union health and safety representatives play in public health. This study addresses attempts by employers and governments to directly or indirectly enforce vaccination for workers, in particular health and care workers. It captures the responses of workers and trade unions to such efforts and implications for employment relations and longer-term occupational health and safety. While national governments have backed away from mandatory vaccination, workers have voluntarily and involuntarily left their jobs in the face of compulsion and employers have used the removal of occupational sick pay and health insurance as coercive mechanisms. The removal of requirements in the UK to self-isolate has raised further questions about non-qualification of low paid workers for sick pay. The research is based on two comparable cities, Manchester, New Hampshire in the US and Oxford in the southeast of England.
Summary
The importance of work and the workplace
In understanding vaccine behaviour, it is not possible to ignore the experiences of frontline workers during COVID-19 and their exposure to the virus. Respondents in Oxford (UK) and Manchester (US) testified to occupational segregation on the basis of ethnicity with BME/BIPOC workers more likely to work throughout the pandemic and to be on non-standard contracts where they did not get paid if they did not turn up for work. The workplace is a key site of infection and prevention and thus key to public health. The perception that government and employers had not protected frontline workers, and a related feeling of being undervalued, appears to have informed subsequent vaccine behaviour. This is supported by UK survey data that indicates perception of economic risk in relation to work is a significant determinant of attitudes toward COVID-19 vaccination. Further, trust in management, but also perceptions of safety in the work environment, both influence attitudes to vaccination and point to the importance of workplace health and safety policies. The survey suggests the necessity of work-related variables in exploring vaccine hesitancy.
A review of occupational and statutory sick pay
Many frontline workers had no recourse to adequate sick pay and leave when symptomatic and continued to work for financial reasons, often under pressure from employers. Those on non-standard contracts have limited or no employment rights. Again, existing exposure to infection affected subsequent orientation to vaccination. More recent coercive policies by US and UK employers, such as withdrawing sick pay from those that are not vaccinated, appear particularly pernicious in a context where inadequate sick pay contributed to the spread of the virus. Based on the experience under COVID-19 there are fears that withdrawal will mean workers are less likely to disclose infection or take sick leave.
Trust in government
Low levels of trust in government constrain the capacity to mobilise behaviour that supports public health and the politicisation of vaccination represents a particular barrier. Participants in this research emphasised that vaccine hesitancy, above all, reflects trust. One Oxford respondent described it as being ‘about your relationship to the state and public health’ and another from Manchester emphasised that ‘trust is the basic denominator for providing any service.’ The survey suggests that neither frontline worker perceptions of public officials’ expertise nor trust in authority affected attitudes towards the vaccine.
Moving away from mandatory vaccination
In both the US and UK, governments have moved away from mandatory vaccination, suggesting that this is not a viable response to vaccine hesitancy. In the US the move reflects political polarisation, while in the UK the labour market is a key factor, namely severe staff shortages in health and social care that predated but were amplified by COVID-19. UK trade unions rejected mandatory vaccination. US union responses were more varied, but they have asserted their right to bargain over the mandate to ensure there are no contract violations. In both countries, trade unionists reported walking a fine line between encouraging and informing about vaccination and supporting those that opposed vaccination.
The threat or reality of mandatory vaccination led to some workers in both Oxford and Manchester leaving their jobs in health and social care or being vaccinated in order to remain in work. Social care workers reported that employers disregarded the earlier requirement for vaccination because of staff shortages.
Migration and refugee status
In both Oxford and Manchester, undocumented migrant workers and refugee communities had particular concerns about vaccination. The UK ‘hostile environment’ and ‘no recourse to public funds’ discouraged migrant workers from getting vaccinated. Similarly, in Manchester it was reported that those without documentation had fears about being asked for identification. Here the move to local vaccination centres that did not require registration or documentation was crucial.
Legacies of racism and discrimination
For BME/BIPOC communities in both Manchester and Oxford, mistrust was historically rooted, with respondents citing medical experimentation on Black populations and communities, including the Tuskegee study of syphilis and AZT trials conducted on HIV-positive Africans. Mistrust was reinforced by more recent experiences and perceptions of racism. Addressing residual inequality in healthcare is a key challenge.
Challenging the racialisation of vaccine behaviour
While legacies of racism fuelled mistrust, at the same time a number of respondents in both countries challenged the view that BME/BIPOC communities were more likely to be vaccine hesitant and felt that the discourse has been racialised. In the US, political factors were as likely to be cited in terms of the White population.
Community outreach
Respondents in both Manchester and Oxford provided evidence of public health outreach campaigns to encourage vaccination. Effective campaigns were based on access to ‘hard to reach services’ rather than targeting so-called ‘hard to reach communities’ and on ‘informing’ rather than ‘promoting’. Bringing vaccination to the community rather than expecting them to go to vaccination centres was deemed important and the opportunity for open dialogue with local health professionals with relationships to communities was effective.
Oxford and Manchester
The research is based in two cities, Oxford in the UK and Manchester in the US, comparable in terms of socio-demographic characteristics. Manchester is New Hampshire’s largest city with a population of 116,000 and is diverse with 10 per cent of the population Hispanic or Latinx. As a gateway city, Manchester’s population includes many migrants and refugees. Those born outside the US, according to the 2020 US Census, comprise 14.5%. This is likely an undercount, as those residents without legal papers are less likely to participate in the census. Manchester has 39% of the homeless population in NH and these are disproportionately people of color.
Oxford is an ethnically diverse city of 151,000, best known as a historic university city, but also the home of the Astra Zeneca Vaccine. Social and health inequalities are evidenced by the fact that men in Northfield Brook, one of the poorest wards in Oxford, die on average 15 years younger than their counterparts living in North ward, one of the city’s most affluent areas.
Walking weapons
Oxford, UK
‘So it was when you cough, when you feel a headache, when you’re told don’t come to work because you may be having COVID. But some of us, we had all those symptoms and still came to work, because as I’ve said, at times you pick - is it my work or is it my bills? Because you’re only paid when you work, when you don’t work you’re not paid. So I think some of the repercussions were people lost jobs, people lost lives, people got depressed and there was nobody to turn to. Then it was, I think it was unsaid, it was silent, it was subtly said “you have to come to work or you lose your job”. Then you get that most people who work in these care places really are migrants, so you see as a migrant also your papers may not be read, or you’re being sponsored by that person. Others were getting COVID, after three days they come to work, then one week later they are sick, they go back, you know, like in-off, in-off. The boss would call them and say, “No you have to come in, we are short, come in.” But you can see they’re not okay.
Some of us when we are positive, you can see that it is actually positive, but some of us we are walking weapons, you can never tell whether I’m sick or not. So at that point in time, some people may have got away with it because they really had no symptoms and they needed to work. Until this PCR testing came in, that’s the time now you hear because you take a test today, and then within the next week two or three people are off sick, they are positive.’
– Oxford Social Care Worker
Manchester, US
'So, who got sick? Folks that got exposed to the virus and who got exposed, the ones that had to show up to the job so they can get a pay cheque. So, there were a lot of people at work, and you become sick then you have to leave. And you have to leave because you can't go back sick and infect everybody. Some folks had vacation time, others didn't. I would say the majority of them did not. You know our employment system in the United States is kind of divided between, we have jobs that are good jobs, union jobs, even if the pay is low you have benefits and time and leave and all that. Then you have the jobs that you get paid when you show up, if you don't show up you don't get paid. It's almost at will and there's a lot of people situated like that, and when that happens it affects folks disproportionately. If you are in a job where if you get sick you're already exposing yourself, doing a job that other people don't want to do and you're showing up when other people are staying home. Then if you get sick, you get penalised for getting sick. In a way, it's unfair like that because you can't go back to work. So yes, it did affect the immigrant population folks with diverse backgrounds differently. And this is not so much as race, but I would say it's because of economic standards, economic status.
– Government health programme administrator, New Hampshire
The study and research methods
The study that this policy briefing is based on asked the following research questions:
- What are narratives and dialogues around vaccination in workplaces and the wider community?
- What are the factors informing vaccination take-up or hesitancy for front-line workers?
- How are organisational rules on vaccination experienced and perceived and how do they impact on recruitment, disciplinary action and workplace exit?
- How do trade unions negotiate organisational rules on vaccination?
- How far have trade unions and community organisations sought to influence attitudes and responses towards vaccination and how have they done so?
- What is the role of health and safety representatives and community activists in influencing attitudes and responses towards vaccination and how has this manifested?
- What are the key influences on vaccination take-up and what are the most effective means of engaging workers in vaccination programmes?
Research methods
The research is a comparative study that focuses on four sectors employing frontline workers in Oxford in the UK and Manchester, New Hampshire in the US. The four sectors are:
- the social care sector
- the health sector
- public transport
- emergency services.
The research is based on:
- documentary evidence of policies towards vaccination
- interviews with key informants
- in-depth semi-structured interviews with workers in each sector
- focus groups of workers in each sector and of community and trade union activists.
Respondents were offered a £25 or $35 giftcards for participation in interviews and focus groups, reflecting the fact that they are likely to be low-paid and time-poor.
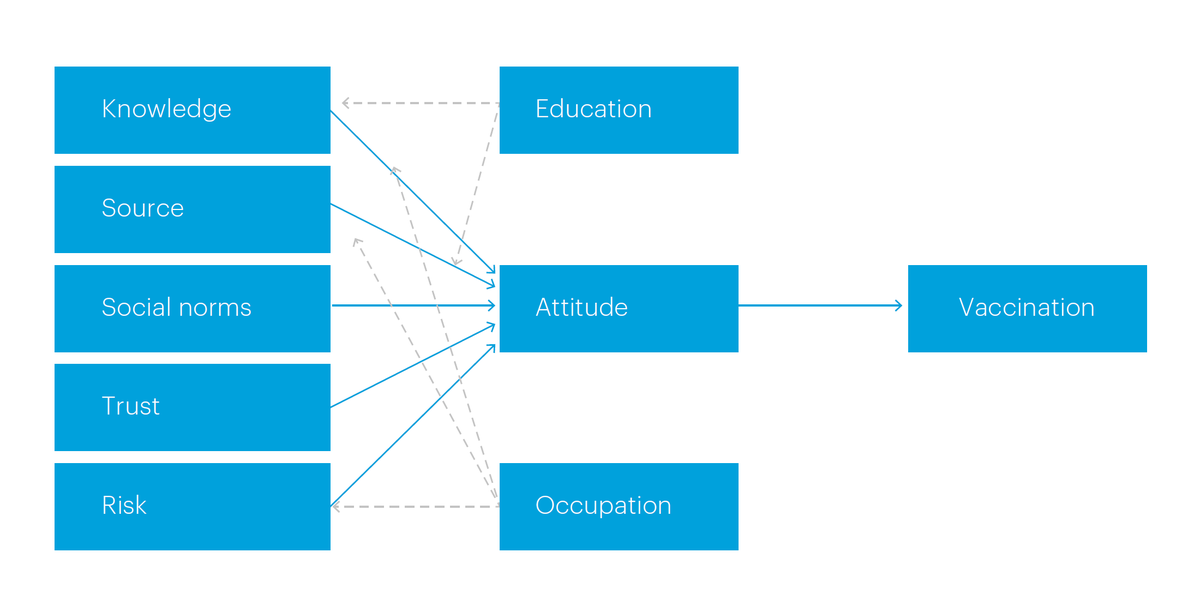
An online survey of frontline workers recruited through focus groups and interviews that aimed to achieve 120 responses each in Manchester and Oxford. The survey is based upon a model of vaccine hesitancy in workers drawing on the Theory of Planned Behaviour (TPB)(2)gas set out in Figure 1. TPB is a psychological theory that links attitudes, subjective norms, and perceived behavioural control to behavioural intentions. Questions pertaining to independent variables (economic risk, affective trust, social environment, safety in the work environment, trust in management, health risk, public official knowledge, trust in authority, and people’s knowledge about COVID-19) and the dependent variables (people’s attitude toward COVID-19 vaccine and vaccination action) were developed to test the hypotheses.
Initial analysis of the survey is based on 170 workers, with 87% from the UK and 13% from the US – returns from the US were much slower and thus the analysis is of a preliminary nature. The majority of respondents (81%) defined themselves as frontline workers and 38% were female and 61% male. They were employed mainly in health and social care (44%) or transport (36%) with 5% in emergency services. Just under half (48%) had tested positive for COVID-19. The reliability test (Cronbach Alpha test) shows a measure of internal consistency and strong reliability scores. While numbers are small and UK respondents predominate, the preliminary analysis indicates the importance of including measures of economic risk related to work in models of vaccine hesitancy. Key individual results are discussed throughout the findings.
Figure 1: A model of vaccine hesitancy in workers
Data analysis of interview and focus group material combined broad comparative understandings across the cases with deep, thick analysis of each case. The material was initially analysed using thematic coding with the support of NVivo software to identify the broad patterns of meaning across data sets. Additionally collective inductive analysis across the research team ensured thematic coding methods did not remove meaning units from the context in which they emerged and highlighted vaccination narratives.
In the UK, key informants included a Trades Union Congress national equalities officer; national officers from transport and firefighter unions; a member of Citizen’s UK’s social care workers’ organising team; a representative from a social care worker support network; a hospital manager and representatives of a local BME community group and national BME nursing association.
In the US, key informants included a senior administrator at one of the two hospitals in Manchester; a senior administrator of a federally funded health clinic; union officers; staff from housing agencies; a senior police officer and fire chief and representatives of migrant and refugee women’s organisations.
In the US, the fact that the hospitals are not unionized made access to workers more difficult – in contrast a number of UK respondents were recruited through trade unions recognized in NHS hospitals.
While in the US nearly three quarters of the respondents were female, in the UK they were more evenly split between male and female. All but two of the UK respondents were BME; of the US participants just under two thirds were BIPOC.
Research was subject to ethical approval by both the University of Greenwich and Southern New Hampshire University Research Ethics Committee. It was conducted on the basis of informed consent with anonymity and confidentiality guaranteed. Data protection follows GDPR and University of Greenwich and Southern New Hampshire University protocols. Case study organisations are not named.
Comparative overview
4.1 The differential impact of COVID-19
Frontline essential workers were disproportionately exposed to COVID-19 in both the US and UK. Evidence suggests that in both countries, BME/BIPOC and migrant workers were more likely to be frontline or essential workers and thus more vulnerable to infection. In the US a Guardian report identified 3,600 healthcare worker deaths between mid-March 2020 and April 2021, with Black Americans disproportionately represented.(3) More than a third of the health care workers who died were born outside the US. Of the deaths identified by country of origin 18% of US health worker deaths were Filipino.
According to the Covid Tracking Project and the Boston University Center for Antiracist Research, Hispanic/Latinx people in New Hampshire were most likely to have contracted COVID-19, and Black/African-American people were most likely to have died from it. Hispanic/Latinx people represented 7,308 cases per 100,000 people, and White people 2,189 cases per 100,000. Black people accounted for 65 deaths per 100,000 people — the highest among any racial category. The figures reflected national trends - people from communities of Color were three times more likely to be infected than Whites and twice as likely to die.(4)
In the UK, Public Health England reported that 63% of healthcare workers who died from COVID-19 were from a BAME background. (5) Figures from the Runnymede Trust found that one third of BME people (33%) worked outside their home compared with closer to a quarter of White people (27%).(6) Just under three in ten BME people (28%) were key workers, compared with closer to two in ten White people (23%). Black groups were particularly likely to be classed as key workers (34%), with the highest percentage among people of African origin – nearly four in ten of whom were key workers (37%). A 2020 study conducted by Oxford University Hospitals Trust recorded the Trust’s porters and cleaners had the highest rates of infection and accordingly BME staff were at greater risk, with job role a proxy for socio-economic background. In the second wave deaths were concentrated amongst those in the poorer parts of the city.(7)
4.2 Vaccination
The US Centers for Disease Control and Prevention (CDC) reported that as of 28 February 2022, 73.4% of people in the US aged 12 and over had received two vaccine doses.(8) On the same date, the UK Office for National Statistics (ONS) reported that 85.2% people aged 12 and over had received two vaccine doses.(9) Although these data suggest that are high rates of vaccination in both countries, there are differences in vaccine uptake on the basis of ethnicity and occupation.
The CDC estimated the percentage of people 18 years and older in US ethnic groups that were fully vaccinated (i.e., 2 doses).(10) It reported that the Asian group was most likely to be vaccinated (96.4%) and that the American Indian / Alaska Native group was least likely to be vaccinated (71.6%). The estimates for other groups were Hispanic/Latinx (83.2%), Native Hawaiian or Other Pacific Islander (NHOPI) (83.6%), White (82.6%), and Black (80.3%). These data suggest a marked difference in vaccination rates between Asian Americans and other groups, but not necessarily between Hispanic/Latinx, NHOPI, White and Black groups. In both countries while White groups had higher vaccination rates than Black groups, in the US the difference between the two was smaller (10%) than in the UK (17%).
The Office for National Statistics (ONS) investigated the percentage of people aged 18 years and older in UK ethnic groups who had received three vaccines.(11) The White British group (68.4%) was most likely to have had three vaccinations followed by the Indian (65.3%) and Chinese (64%) groups. The Black African (37.9%), Pakistani (37.8%) and Black Caribbean (33.9%) groups were least likely to have received three vaccines, with half (50.4%) of the ‘White other’ group having done so. While ONS figures (12) confirm that particular ethnic groups were more vaccine hesitant, they also show that the proportion of adults who received three vaccinations was lower for those living in more deprived areas, who have never worked or were long-term unemployed and who identified as Muslim compared with other religions.
Differences in vaccination rates have also been found between UK occupational groups. ONS data shows that workers in the hospitality, personal services and transport sectors were less likely to have received a vaccine than workers in other sectors.(13) Among those aged 40 to 64 years, over 80 per cent of health professionals had received three vaccinations. The occupations with the lowest proportion of people with three vaccinations were elementary trades and related occupations (58.3%) and skilled construction and building trades (62.3%). Data from a UK NHS trust showed significantly lower COVID-19 vaccination rates among ethnic minority healthcare workers (71% in White workers compared to 59% in South Asian and 37% in Black workers).(14) Further evidence suggests there may be avoidance by those who work in lower paid public facing roles.(15)
4.3 The political framework
In January 2022 the US Supreme Court rejected President Biden’s plans for compulsory vaccination or testing for 100 million workers, about two-thirds of the American labour force, including federal government workers. All US companies employing more than 100 people would have been required to ensure that their staff were fully vaccinated or took weekly COVID-19 tests. The US Supreme Court allowed the Centers for Medicare & Medicaid Services (CMS) to proceed with the directive in states that challenged the rule.(16) The CMS rule applies to health care workers in Medicare and Medicaid-certified providers and suppliers, covering roughly 50,000 providers and 17 million healthcare workers. Central government employees are also covered, with the Biden administration urging state governments to follow. A number of states required vaccinations for teachers and school staff. Companies, such as McDonald’s, Delta Air Lines, United Airlines and Tyson Foods, require either vaccination or regular testing among their US workforces. However, Starbucks rescinded plans for mandatory vaccination.
In the US, vaccination is thus highly politicised, with narratives revolving around personal freedom. Governors of Republican-led states pledged to challenge executive orders in court with the governor of Texas, Greg Abbott, calling the regulations ‘an assault on private businesses.’(17) In the UK, there has been broad consensus across the main political parties and the issue is less politicised. The government amended the Health and Social Care Act 2008 to mandate vaccination for care home workers from November 2021 in England. It was estimated in July 2021 that care homes faced losing 40,000 staff from the compulsory vaccinations policy. Discussions with key informants suggest that this fear materialised and there has been some exodus. However, on January 31st the UK government removed vaccination as a condition of working in care homes and reversed its plans for mandatory vaccination for NHS staff in England (devolved governments in Scotland, Wales and Northern Ireland had no plans for a mandate). The move came three days before the 3rd February deadline for unvaccinated staff dealing directly with patients to have had their first dose or risk losing their job. The decision came in the face of warnings by medical bodies that the government policy would exacerbate chronic workforce shortages in the health service by causing thousands of staff to lose their jobs. The health minister, Sajid Javid, cited shifts in risk from the omicron variant and that the population was better protected against the need for hospital admission. Government figures showed that five per cent of NHS staff remained unvaccinated (80,000).(18) Data from NHS England stated 91.5% of NHS trust healthcare workers had received two doses of a COVID-19 vaccine as of 13th January 2022.(19)
4.4 Employer responses
A February 2022 New York Times survey of 500 top US employers found that 75 of the 120 that responded required vaccinations for some of their workers; 36 deferred to government mandates at the local, state and federal level; 18 had no plans for mandates. There were another eight corporations that did not respond, but had some employees subject to the federal mandates for health workers. In the firms mandating vaccination, seven required boosters, five indicated that they would offer regular testing as an alternative and 12 reported that they would be disciplining or terminating unvaccinated workers.(20) A number of large employers have altered sick pay for unvaccinated employees.(21) Delta Airlines had imposed a $200 monthly insurance charge on employees on the company insurance plan who were unvaccinated. Others were restricting returns to the office to vaccinated workers only and requiring that all new recruits be vaccinated. Columbia Sportswear had put unvaccinated workers on unpaid leave and begun termination processes. However, meatpacking firm, Tyson Foods, negotiated with unions to provide paid sick leave as an incentive for vaccination with the United Food and Commercial Workers (UFCW) stating it is the first national US agreement to provide paid sick leave to meatpacking workers. In New Hampshire, as elsewhere, the firefighters’ union pushed for the government to provide money for sick pay in order that firefighters did not have to utilise existing sick leave.
In the UK, in the context of staff absences and shortages, there was also a move by employers to cut sick pay for unvaccinated staff. In January Morrisons, Wessex Water, Next, Ocado and Ikea cut sick pay for unvaccinated workers who are forced to isolate after being exposed to COVID-19, leaving them dependent on SSP. The legality of the trend has been questioned, particularly in terms of the UK Equality Act where vaccination status may be an outcome of pregnancy or religious or philosophical beliefs. However, other opinions are sceptical that employers can be challenged on the grounds of discrimination as vaccine hesitancy is "unlikely to be a protected belief for the purposes of the Equality Act". There are fears it will mean employees are less likely to disclose infection or take sick leave.(22) As in the US, there are cases where UK unions have negotiated improved sick pay as a result of COVID-19 – the RMT transport union, for example, pushed for full pay from day one for cleaners working for private contractors on London Underground.
Research findings
5.1 The importance of work and the workplace
The experiences of frontline workers who worked throughout COVID-19 were salient to vaccine behaviour. Such respondents reported feeling unprotected and undervalued during the pandemic. In Manchester, a Community Building Manager described how some tenants were working in close quarters on the factory floor, with not all wearing masks the whole time. A number had contracted COVID-19 more than once. The Service Employees International Union (SEIU) reported that janitorial workers were being told to reuse the same mask for eight-day periods when cleaning rooms that had been occupied by COVID-19 patients. In Oxford, it was reported that initially care home and agency staff worked without adequate PPE.
There were indications of occupational segregation by race and ethnicity in both Manchester and Oxford, with BME/BIPOC workers more likely to be key or essential workers. A pastor representing women from the refugee and migrant community in New Hampshire noted:
“First of all, there was a lot of things affected the community. When this COVID was very bad, what we really was scared about, because the African people was working a lot, they was working a lot because they say like they give them double, you know? And most of the people refused to go to work, but the African people was working a lot. And some places they was not like helping them to be protected themselves, you know? And they just let them.” (USKI3)
In Oxford, a transport worker commented:
“The Black and Ethnic Minority community has been badly affected. First, it was because most of the people are on the frontline. The cleaners, nurses – because the NHS employs quite a lot of our Black and Ethnic minorities. And the accommodation that they have, because they will normally share accommodation. Our culture is such a way that you have to stay with maybe your mother and your other brothers and everything. And because of the low wages that most of the people earn, it means that they will stay in intergenerational areas.” (UKFG3)
The deaths of BME porters in one of the Oxford hospital trusts in the early stages of the pandemic was formative for a number of healthcare respondents. Similarly, another respondent recalled the deaths of 60 Filipino healthcare workers across the UK. There were perceptions of differential treatment of workers during the pandemic. In healthcare in Oxford there were stories that BME nurses were pushed into the frontline and more exposed to COVID-19. BME care workers felt that White workers were less likely to be pressured by employers to attend work or threatened with overall cuts in hours if they turned down specific shifts. In one Oxford hospital it was noted that an inspection had flagged that there were issues with social distancing for lower-paid housekeeping staff, more likely to be migrant workers, who had much smaller changing and washing areas and facilities than nurses in the same hospital, who were more likely to be White and/or British.
Respondents referred to contractual differentiation where BME/BIPOC and migrant workers were more likely to be on contracted-out or agency contracts, while working alongside directly employed White workers. Across the US the SEIU reported the increased use of staffing companies and contract labour to supplant full-time workers. In the UK there were particular impacts on those working in contracted- out or privatised services and on non-standard contracts with fewer employment rights and who were not paid if they were sick. In transport, one respondent reported the use of agency workers in customer service roles who did not get paid if they did not come into work. He recorded the anxiety of directly employed workers working alongside them, since agency workers travelled between work locations with the risk of spreading the virus.
Respondents felt that workers without employment rights, particularly if English was not their first language, often felt scared of losing their jobs and thus being open about COVID-19 symptoms, of turning down work and challenging employers. A care worker reported fears among colleagues of joining unions. In Oxford, a union representative reported that East Timorese workers had seen colleagues fired if they raised concerns and emphasised the difficulties that someone on a zero-hours contract, dependent upon their employer for hours, would have raising health and safety issues.
The survey suggests the importance of workplace health and safety to worker attitudes to vaccination, with affective trust in management (p=.015), and perceptions of safety in the work environment both significant (p=0.40).
5.2 A review of occupational and statutory sick pay
Experiences of frontline workers were intimately linked to access to sick pay and leave in both the US and UK. Many respondents reported that frontline and lower-paid workers attended work when symptomatic because of their limited rights to both occupational and statutory sick pay, with the latter inadequate to support families. This was particularly the case for those on non-standard contracts. In the US, those with COVID-19 were increasingly expected to use unpaid leave if sick leave ran out. In the Box on page 4 above, an administrator on a government health programme in New Hampshire reflects on the concentration of the migrant population in lower-paid, frontline jobs and, by implication, the absence of sick pay.
A Community Building Manager for low-income families in Manchester reiterated the pressure workers were under to return to work after COVID-19, using the example of a factory worker originally from Bosnia who worked 50-60 hours a week and spent eight weeks in hospital with the virus. Since he was supporting a household he returned to work, but for a maximum of 25 hours a week because he could not stand for too long and had breathing problems. He then got COVID-19 a second time and was out of work: "so just people that weren’t necessarily in the healthiest conditions really struggled long term and we’re seeing people get COVID more than once because they have to go back to work." An SEIU respondent suggested that workers were given conflicting messages by supervisors and managers as to how long to take off work and many felt pressurised to return early, particularly where services were short-staffed.
The union had demanded that hotel rooms and childcare were paid for in the case of workers who had to stay away from their family members while they continued to work in healthcare. On the other hand, an officer from the Manchester Police Department confirmed that if officers needed to quarantine, the city initially allowed 14 days that did not impact on sick leave. Subsequently, such time came out of Family and Medical Leave, but there was a broader approach that encouraged officers to take sick leave if they had to without negative consequences.
In the Box on page 7, an Oxford care worker provides a harrowing description of working through COVID-19 and how the lack of protection and employment rights for care workers spread the virus, suggesting why deaths were so high in care homes. Under-staffing meant she often had to cover for her colleagues’ sickness and she powerfully conveys the pressures to work when symptomatic, particularly for migrant workers, as well as the fear of raising issues. She was paid £40 by her employer for each of three periods of COVID-19 sickness. She describes care workers as ‘walking weapons’ and that the lack of widely available testing in the early stages of the pandemic allowed people to work when symptomatic. Other care workers reported that they may not even qualify for the statutory minimum sick pay. An Oxford community activist said that East Timorese workers with no access to sick pay worked throughout the pandemic. In one case, nine were sharing a house and all were going to work with COVID-19; ‘they had to pay their rent’. An Oxford union rep also noted that migrant workers did not come forward for testing because they could not survive financially if they tested positive and had to go off sick:
And that’s really where the whole system falls down, it’s because if you can’t make ends meet you’re just going to continue working even if you don’t feel well. And that’s not good for the individual but it’s also obviously not good from a public health point of view. And that has never been treated as a public health issue, but it was absolutely clear in the pandemic that it is a public health issue. And that’s why the lowest paid workers were the most at risk. They had the highest risk because it is a public health issue when you are working in conditions that do not allow public health initiatives to have any meaningful impact.” (UKKI2)
A porter at one of the Oxford hospitals reported that while directly employed porters were paid as normal if they went sick, agency porters had no access to occupational sick pay and were reliant on SSP, which they could not live on, resulting in them coming into work sick. He pointed to the unfairness of having agency and directly employed staff working side by side, but treated differently. He also said that there were rumours that the Trust wanted to replace all directly employed staff with agency porters because such employment rights made them "too expensive". Respondents also linked burn-out as a result of working through COVID-19 to long-COVID. Care workers talked about silence around long-COVID, particularly by employers anxious to keep them at work.
The experiences of frontline workers, including the lack of PPE and sick pay, were explicitly linked by a number of respondents to subsequent vaccine behaviour as an Oxford care worker put it:
“I think from having just spent time talking to people, it’s more about the fact that if you don’t feel cared for by your employer and then suddenly they’re saying “come and do this thing because we want to care for you to protect you”; you think “well, you’ve never cared for me before, why will I believe that you’re doing this for me now?” Does that make sense? But between the residents and the institutions, the public sector, there has to be a two-way trusted relationship for this to work. And when you have always felt that you were not cared for and you were just there to do your job and not make any fuss, then why would you then suddenly believe that what you were being offered was for your benefit and not for other people’s benefit?” (UKW5)
An Oxford Hospital consultant and union rep also discussed the impact of the one-sided employment relationship where BME frontline workers felt that their health and safety was not being considered during the pandemic, leading to suspicion when "suddenly we are being asked to rush to the front of the queue" for vaccination. He also proposed that BME staff "had racist experiences when they had accessed healthcare themselves. And I understand that degree of, not just mistrust, but also the question comes into your mind, 'what is the employer trying to get from me that they want me to have this vaccine?' (UKK12). A senior manager in an Oxford health trust suggested that the exposure of frontline workers to infection during the pandemic could foster a view that they had immunity:
“I was talking to some colleagues and friends and their argument is, 'if I am wearing PPE, I wear a mask, I wear gloves, then I cannot infect other people and I cannot be infected because I am protected with the PPE'. And he said that during the height of the COVID-19, during the first and second wave, they don’t have the vaccine [and] they did not infect or they were not infected. And that’s their argument.” (UKKI4)
Survey data indicates that perception of economic risk determines attitudes toward vaccination with an inverse relationship between vaccine-taking action and perception of economic risk (p=.016). This suggests that workers who were worried about not getting sick pay or not being able to work due to COVID-19 were more likely to have negative attitudes towards vaccination. The implication of these findings is that mandatory vaccination is not likely to work. Nearly half of respondents (48.8%) stated they were worried or very worried that they would not get sick pay if they got COVID-19 and just under two-thirds (62.3%) that they would not be able to work if they did so.
5.3 Wider narratives - trust in government
The survey suggests that neither frontline workers’ perceptions of public officials’ expertise nor trust in authority affected attitudes towards the vaccine. Instead, social environment and the influence of peers are more important (p=0.001). The politicisation of vaccination in the US is reflected in the interview data. As one Manchester trade unionist put it:
“In my opinion, vaccine hesitancy comes from a couple of different sources or reasons. Unfortunately, the biggest one is political. And we are a divided country right now. And depending on what side of the fence you’re on, it’s probably going to dictate some of your attitudes towards vaccines and vaccine hesitancy.” (USKI8)
A more consensual approach across political parties meant that such polarisation did not apply in the UK, but the government’s performance on COVID-19 did inform UK respondents’ narratives and influenced trust. A participant in the public transport focus group commented:
“The lack of trust for this specific government as well is so high across all boards. And time and time again we are just seeing – they’re showing themselves for who they are, that they’re untrustworthy. I think there’s a lot of people now that just distrust – and I think I was listening to a medical academic speak about this. He was saying when you have a government like this, that it’s so distrustful and it is quite harmful to public health. So, it’s really scary times we’re in I think to be honest.” (UKFG4)
In the US there has been more industrial conflict over vaccination, including the termination of municipal contracts in New York and protests by firefighters and police. A New Hampshire fire chief understood that 3,000 of 12,000 firefighters had retired in New York City ‘because their ultimatum was “listen you get the vaccination, or you resign or retire”’. Some US trade unions are more cautious in their response than UK unions, not wanting to step ahead of their members in advocating vaccination. While a number of unions have encouraged vaccination, the Service Employees International Union (SEIU) representing health and public sector workers and the United Steelworkers union (USW) were opposed to mandatory measures. Some state courts and agencies have concluded that state and local government employers are not required to negotiate with unions over vaccine mandates because it’s an urgent health emergency. In response unions have asserted their right to bargain over the mandate even if they support mandatory vaccination or have no policy, in order to ensure there are no contract violations.(23) One US trade unionist identified the tension between supporting members and promoting vaccination:
“There’s still a group of 35% maybe of people that just don’t want to be forced by their employer to do something, or the government. It’s not up to us to police people’s lives, it’s up to us to protect their rights under the contract, protect their civil rights if we can. But it’s not really up to us to push people – they have the ability to make their own decisions. It’s a really hard line to walk when you believe 'just take the damned shot and put your mask in', it’s hard to say that to people sometimes. If you’re asking my opinion, the members – I give them my opinion and there’s never been a doubt about my opinion on things. But I represent people all the time that do things and I just shake my head and do the best I can to mitigate whatever the circumstances are afterwards.” (USKI7)
In the UK national trade union reluctance to back mandatory vaccination reflected concerns about residual and COVID-19-related staff shortages in health and social care. This fear was reflected by a senior manager at an Oxford Health Trust:
“So the question is, can we afford, can the government afford to lose the 70 to 80,000 healthcare workers? What will happen to the NHS? And I am fully vaccinated, I have my booster dose, I’ve done a lot of campaigns, but I respect people’s views, people’s opinion. At the end of the day it is their human rights and my personal view is it must be respected. Of course, we educate them and encourage them. Exactly the same as our patients, we cannot force patients to take the treatment because simply we believe that it’s the right treatment for them.” (UKKI4)
While advocating a programme of education and encouragement, unions at national level asserted that making vaccination a condition of employment constituted an infringement of worker and human rights. One UK national trade union representative perceived mandatory vaccination as shifting responsibility for workplace health and safety from employers to individuals. The Oxford focus group of public transport workers – a highly unionised sector – reflected on how trade union reps had ‘conscientized workers’ to challenge management on health and safety and ‘keep them on track’ during the pandemic, as one participant put it, "they were intrinsic with how my organisation dealt with Covid. I honestly feel that if we didn’t have a trade union within my workplace, I feel like it would have resulted in the loss of lives in regards to the pandemic." (UKFG3).
As in Manchester, local trade unions reported difficulties in walking a line between encouraging vaccination, but also supporting those who rejected mandatory vaccination. One focus group participant from of a BME self-organised group in Oxford said that making vaccination ‘a condition of deployment’ (the term used by the UK Government) had been discussed by the union regional meeting which concluded that it could not take a position one way or the other:
“[The union] doesn’t want to actually force its members, we want members to decide. So that is information we passed on to our members. But when the government came up with this draconian decision, a law that everybody should get the vaccine - everyone that has not had the vaccine are panicking. They were asking a lot of questions, especially directed to [union] reps. It was very traumatic during that time until now. But I’m not directly affected anyway but because I had my Covid vaccine. But people who didn’t want to have it, they felt that they were being intimidated and being forced to have it. So that is how people feel. I don’t think there was much any [union representative] could say with the condition of deployment. So based on the government putting that down as law, no [union representative] was in a position to be able to really say 'yeah or nay' kind of thing. You can’t say 'don’t have it', because you will be giving advice which might result in them being unemployed or redeployed to a lesser degree. Or you shouldn’t be in a position to be able to scaremonger them and encourage them to have it because that would be the wrong thing as well. I don’t think any union representative was in a position to be able to do anything within that, other than maybe just emotionally support somebody that was maybe struggling with making a choice. The choice is still going to be theirs; it would be foolish of any union representative or official to push one way or another.”(UKFG2)
A second member of the focus group reported that the union had discussed the condition of deployment policy with management in the Trust and how to support unvaccinated staff, including setting up drop-in sessions for those unsure and who had questions. Another Oxford respondent stressed that trade unions had a role in the provision of information because of their independence from employer interests. In the public transport focus group, a participant told how she had felt her union’s stance on vaccination was initially not culturally sensitive:
“I think we spoke about the importance of having health and safety reps that represent all the demographic of the union. I think at first some of the language was very – 'yes, all members should be vaccinated blah blah blah'. Because of maybe they weren’t culturally sensitive to different perspectives. And that was quickly shut down, I know within my union obviously because I represent Black and Asian and ethnic minority members. And so, there was a few of us at those meetings when we had a district wide meeting. Where we were like 'listen, that’s not your place, that’s not our place. We can’t be seen to be pushing that narrative, that’s not what we’re here for. Like you said, you’ve got Public Health England or whatever to do that. We have to represent all members, whether they want to or not and it’s not really our position – we’re not in a position to be questioning or putting our personal views on to our members.' But I do think it was something that had to be pointed out because they didn’t really realise the nuance in regard to dealing with certain communities that may have that suspicion and mistrust.” (UKFG3)
5.4 Moving away from mandatory vaccination
Both national governments had subsequently retreated from compulsory vaccination and there was no mandate in New Hampshire as the state of New Hampshire itself was party to the challenge to the Biden presidency on the issue. Manchester workers thus appeared less likely to feel that their jobs were at risk. An exception was in the US health focus group where it was reported that there was mandatory vaccination for healthcare workers in one hospital from January 2022. Here there had been resistance from some employees, some of whom resigned prior to the implementation of the mandate. Those who objected had to apply to Human Resources and were "reviewed by a committee" that could grant exemption on ethical or religious grounds or on the basis of workplace environment concerns. Those not granted exemption, "a handful of staff", had their contracts terminated, deemed by the Hospital as "voluntary resignation". As one participant put it, "people were not happy." In another organisation, a respondent reported that his employer gave an incentive of $500 or five extra paid days off if staff got vaccinated.
Respondents from Oxford reported that prior to the change in government policy, the local Council had written to social care employers stating that care workers had to be vaccinated. Subsequently, the NHS Health Trust had sent individual letters to workers telling them they needed to be vaccinated with their first dose by 3 February 2022 and highlighting that there would be no redeployment if they refused and were not exempt. This was perceived as a threat that workers would lose their jobs and union members approached their union for advice. A number of workers left their jobs in the face of mandatory vaccination or were reluctantly vaccinated to retain their jobs and felt it was forced upon them. At the same time, it was stated that tight labour markets and staff shortages in both Manchester and Oxford made social care employers reluctant to enforce vaccine mandates and that there were cases where they disregarded such requirements. In the US, it was reported that numbers of healthcare workers had left the sector following the pandemic, experiencing burn- out and trauma. A senior manager in a Manchester healthcare centre reflected on the impact that staff shortages had on employer approaches to vaccination:
“We face such incredible workforce shortages right now that the prospect of losing 20, 30, 40, 50 nurses is unfathomable. So we had to come up with a creative way in listening to our employees. And we held listening sessions to hear why people did not want to receive the vaccine or did not want to start a mandatory policy. And you can imagine they were all over the place, some nastier than others. But the question of pregnancy and birth was a big one and we heard that and we put our policy in place to help address that.” (USKI8)
One Oxford care worker noted that formally if she and her colleagues did not take regular COVID-19 tests they would not be put on the rota. However, employers turned ‘a blind eye’ if staff refused to be tested:
“They want the shifts covered. They just want us to do the job, the shifts have to be covered one way or another, whether or not – because a lot of people don’t want it and a lot of people have left. I know a lot of people who have left, but they’re really having staff shortages. They just want the shift covered so if you can cover it, because they don’t have a lot of people, they burn out the few that have it, that are there.” (UKW5)
Another care worker confirmed that while vaccination was needed when applying for care jobs and specified on application forms, employers were less strict with existing workers.
5.5 Migrant and refugee status
In both Oxford and Manchester, it was reported that undocumented migrant workers had particular concerns about vaccination. The UK ‘hostile environment’ and ‘no recourse to public funds’ were seen to discourage migrant workers from registering with the NHS and/or for vaccination. Here the move to vaccination centres that did not require registration or documentation was crucial. Similarly in Manchester it was reported that distrust of the vaccine was compounded by fear of the government within the migrant community.(24) Those without documentation were anxious about being asked for identification, as a worker in a healthcare centre in Manchester reported:
“We have folks who do not have documentation to be here and so they were really concerned about – 'this is a governmental vaccine and if I go and try to get the vaccine am I gonna get deported when they find out that I’m undocumented?' And they were asking initially for a licence or some form of identification and some of the folks that are here that are undocumented, they use another ID to work under, another name to work under that is a legal name than what their real name is. And so, then they were worried about 'what name do I give when I go to get my vaccine?' and 'if I’m giving this other name then the vaccine is gonna be in that name and not in my name.' So it was very worrisome to some folks, especially around documentation issues.” (USKI6)
In response the organisation did extensive outreach work to communicate to migrant workers they would not be asked for identification or documentation and would not have to have their names on vaccine cards. This respondent also acknowledged the role of community leaders in reassuring people. It was clear that requiring online registration for vaccination did not work, with access to technology another factor.
Again, it was opening vaccination centres within the community where people could just turn up and get a vaccine that was effective.
5.6 Trust
The focus groups represented different views on vaccination and sparked lively discussion with individuals reporting differences within their own families and households. Behaviour reflected a spectrum of individual and structural factors, as one Oxford focus group member put it:
“I was just thinking about access to vaccinations, so not only access in terms of being able to get somewhere where someone can put a shot in your arm, it’s also access to relevant information. But it’s about your relationship to the state and public health, and what that means about following government guidance and all of those sorts of things.” (UKFG1)
Hesitancy was defined in terms of personal choice and control over one’s own body, but also extended to worker and human rights. A New Hampshire union representative suggested that union members might be more resistant as they would see compulsion by employers in the context of worker rights and wider industrial relations:
“When people are represented by a union, they have more of a stance, 'they can’t make us do that, can they?' And that’s what people are coming to now, 'can they make you?' Well, people will come to us and say, 'well they can’t fire me, can they?' You say, 'well no, they can fire you, whether I can get your job back is another story'. So, it’s the same type of thing as 'can they force me to?' Well, I don’t know – certainly they’re not going to come to your house and give you a shot, they can’t force you to take it, but what are the ramifications if you don’t take it? If it’s a private business and they own the property, they can tell you that 'I don’t want you on my property.' It’s a tough legal question, it really is. The majority of our members are vaccinated, but the minority of people have the right of dissent. So, you have to respect people’s rights to dissent and as long as it doesn’t cause harm to the people who are in the majority. And that’s kind of where we come in and try to mitigate any actions against them.” (USKI7)
Narratives around vaccine hesitancy, in both Oxford and Manchester were characterised by lack of trust. As a senior manager in a healthcare centre in Manchester put it:
“Trust is the basic denominator for providing any service to that population. Whether it’s primary care, behavioural health, vaccine, name the service and if you don’t have a trusting relationship there is going to be reluctance automatically.” (USKI8)
UK respondents expressed mistrust arising from the Government’s initial ambiguous response to the pandemic. Political scandals surrounding its track and trace system and profits made by private companies from COVID-19, including those manufacturing the vaccine, had not helped. One trade unionist said that her scepticism stemmed from what she saw as the government’s privatisation of the NHS, while a care worker identified ‘the big pharma agenda.’
A proportion of respondents suggested there was a lack of confidence in the science of the vaccine and fears of possible side-effects, including on fertility and pregnancy. In both countries a number felt that the vaccine had been developed too quickly with insufficient research and there may be longer-term outcomes. In Oxford, respondents felt that the media reflected government scaremongering about the impact of the virus. In the US, there was a concern that the vaccine was not approved by the US Food and Drug Administration (FDA).
A small number of participants discussed misinformation including via social media, but also community television channels. A Manchester health focus group reported beliefs that the vaccine could alter genetic make-up, but also that it was part of a ploy by the federal government to obtain information about the population. A worker at a Department of Health COVID-19 centre in New Hampshire, who was herself of African heritage, discussed reluctance in the African community. She referred to the influence of the former chief judge, Justice Mogoeng Mogoeng in South Africa, who on the basis of religious conviction considered the vaccine satanic and also as changing DNA. She was one of the minority in her family who had been vaccinated and repeated the joke from within her community ‘We are waiting to hear that you died because you took this thing’. The representative of a community housing project indicated that for Catholics, objections were based on the belief that the vaccine was made with aborted foetal cells, and she attributed this to coverage by Latinx community television channels. In response, the project targeted information via Whatsapp, text, email and Spanish-speaking media channels.
Respondents also perceived scepticism about booster vaccinations on the basis that they and others close to them have continued to contract COVID-19 variants following initial vaccination. There was a view that vaccination was ‘going on and on with no end in sight’. In one of the Manchester focus groups, a public housing worker expressed the view that initial messaging had made people think they would not get COVID-19 following vaccination and the fact they did (albeit without hospitalisation) had reinforced the anti-vaxxer case.
5.7 Legacies of racism and discrimination
For BME/BIPOC communities in both Manchester and Oxford mistrust was historically rooted, with respondents citing medical experimentation on Black populations and communities, including the Tuskegee study of syphilis (recalled by UK respondents) and AZT trials conducted on HIV-positive Africans. Some respondents identified reticence by BME/BIPOC communities, particularly those from Africa. A participant in a focus group based on an African Women’s organisation in Manchester said there was a fear that vaccination would be imposed in Africa:
“They don’t trust, because they say, “This isn’t for the Black people,” or, “If you take a vaccine, you’re going to turn ghost.” There is a lot of reason why, especially through the media, the social media. But they say they are bringing the vaccine to Africa. If here in America they didn’t find a vaccine, which vaccine they find to bring to Africa? And we started to raise awareness. They don’t trust to take the vaccine, because of all those things what they did, we don’t trust in government for what they say. And people sometimes they don’t trust medicine, they start to say, “They just want to kill the Blacks.”” (USFG1)
A volunteer for an African community organisation in Oxford similarly commented:
“I just know from talking to people that there was a lot of people completely refused to take the vaccination because of mistrust, because of racism, because of previous trials on us and stuff like that. People are thinking “oh here we go again, this is about killing all Black people.” So, obviously there are those kind of feelings there, which they are quite right and they’re quite entitled. Because we always feel that, they’ll say try it on them first and see what happens, so there is that big mistrust that we could never get over.” (UKKI3)
Respondents also objected to the naming of COVID-19 variants as ‘South African’ or ‘Indian’ – perceiving this as racialisation. Residual mistrust was supported by more recent experiences and perceptions of racism. A participant in the Oxford public transport focus group, like others, mentioned the disproportionate deaths of BME women in childbirth:
“I think it’s a lack of trust. I think that there are certain communities that don’t trust the medical practitioners or modern medicine. And I think that when you’re getting the reports that we have had coming out now recently, Black women are four times, five times more likely to die in childbirth than other women. So, I think the care that you receive can be quite racialised. And I think that there is a lack of trust really where people feel they don’t really trust it. And as well as, because of historically there have been so many incidents where we’ve been used, experimented on etcetera. I’ve heard loads of comments like 'why are they pushing it so hard? They never do anything for us.' The kids will be like 'wait a minute, you never do anything to benefit us.' You’re kind of looking at the government suspiciously, kind of like 'oh you want us to be the first ones?'” (UKFG4)
5.8 Challenging the racialisation of vaccine behaviour
While legacies of racism fuelled mistrust, at the same time a number of respondents in both countries challenged the view that BME/BIPOC communities were more likely to be vaccine hesitant and some felt that the debate had been racialised. UK respondents mentioned (White middle class) resistance to the Measles, Mumps and Rubella vaccine, but also hesitancy amongst some Eastern European migrant groups. In the US political factors were as likely to be cited in terms of the White population. An officer from the Manchester Police Department described an anti-vaccine protest at a children’s vaccination clinic by a small group of "generally what we would frame as the free stater populations of a libertarian type population front. And that population, at least from what we see, is primarily White." In the UK an Oxford hospital consultant and union rep stated, "the biggest propagators have been actually the organised and far-right anti-vaxxers who are very well connected and very well-funded actually."
A BME bus driver from Oxford concurred:
“There was that allegation that it was our community. But if you went on social media and saw the marches against the forced vaccination, it was mostly White people. So I don’t know where they were labelling communities with that when there was a far greater consensus of Caucasian people on these marches.” (UKW7)
5.9 Community outreach
Directly employed health workers generally recounted that access to vaccinations was relatively easy. In the US, employers are required to provide paid time-off and trade union respondents emphasised the importance of ensuring workers did not suffer financial loss. In Manchester evening clinics were provided for municipal workers that could not attend in the day.
In both cities, access was more difficult for workers on non-standard, precarious contracts who often worked long hours and were fatigued. Such contracts do not allow ‘paid time-off’ since workers are paid on contact time or presence in the workplace. Workers described long queues for vaccination and having to travel to clinics. A hospital porter in Oxford indicated that he and his colleagues were allowed paid time off to get vaccinated or tested, but this did not extend to agency workers who had to do so in their own time. The lack of access to employer email systems that provided information on vaccination was also cited as a barrier for manual and contracted-out staff.
Respondents in both Manchester and Oxford gave evidence of public health outreach campaigns to encourage vaccination. In Manchester, the city employed four additional multi-lingual community health workers to reach those disproportionately affected by COVID-19. Effective campaigns were based on access to "hard to reach services" rather than targeting so-called "hard to reach communities" and on "informing" rather than "promoting". Such campaigns focused on education, communication and open discussion. In Oxford, the Why Vaccinate project, brought together community organisations, health professionals and local politicians and activists, to share information and to have an honest dialogue. One initiative took the form of an online meeting of the BME community with around 30 BME doctors and health workers from different specialisms where people could ask specifically about vaccination. The close relationship between the trade unions and community facilitated this intervention which then informed the NHS Trust outreach strategy. A community activist described how the Why Vaccinate project overcame her hesitancy and allowed her to play a role in encouraging others:
“I do know that the Why Vaccinate did make a difference in terms of people saying 'I wasn’t going to vaccinate but now I will.' I was one of those that was a sceptic. I think why I was able to push it was because I was one of the sceptical ones. I was thinking 'no way' – but when I saw the doctor saying 'well I’m vaccinated', doctors saying 'I’ve vaccinated and I’ve been well.' So, yeah, for me it also convinced me to vaccinate. I didn’t vaccinate until that happened. So, I wasn’t speaking as a vaccinee at the project, I was speaking as a sceptic as well! So, it gave people respect in terms of not dismissing… as if you are just imagining things. We weren’t saying that people were going to solve the problems of the past, but acknowledgement helps a lot.” (UKKI1)
The SEIU similarly put on a series of informational town hall Zoom meetings led by union leaders on the basis of open dialogue with local health professionals.
Some respondents stressed the importance of targeted and "culturally specific" campaigns. In certain cases, "opinion or community leaders" from within workforces or communities were brought in and were successful where they could communicate in community languages. A community housing project in Manchester distributed information in eight languages. While initially transport had been an issue, subsequently pop-up clinics located in vans were held in the community leading representatives from the Health Department to conclude “Oh, you need to bring this to the neighbourhoods, we can’t expect people are going to come to us.” Since tenants did not all drive the Community Building Manager stated:
“I work really hard to make sure that all of our tenants that still have the hesitancy or say, 'I don’t know where to go', I make sure that we get them as many resources as possible that’s walking distance.” (USKI9)
Similarly, a non-profit organisation representing women refugees and migrants held mobile clinics in its office, with the pastor taking the vaccine herself as an example. In Manchester it was reported that the homeless are most resistant to taking advantage of services and consequently programmes were based in homeless camps in Manchester. Evidence suggests that with one or two exceptions (in Manchester, Pentecostal and Hawaiian churches), churches, mosques and faith networks were key bodies encouraging vaccination, because of the trust they engendered. Local community churches promoted vaccination amongst congregations and clinics were held in some churches. There had also been on-site vaccinations at a local Pride festival. Manchester Public Health partnered with the New Hampshire State Department of Health and Human Services, the Granite State Organizing Project, NeighborWorks of Southern New Hampshire and Fresh Start Farms (a farmers’ cooperative with migrant and refugee members) to organise a fair that located vaccination in the context of wider health issues.
Conclusions
The research suggests similarity between factors behind vaccination hesitancy in both Manchester and Oxford despite the differences in national health systems, possibly reflecting the exceptional dependence on public funding to tackle COVID-19 in both countries. The key variation is the extent to which vaccine behaviour is influenced by political polarisation in the US. This political context may inform higher convergence of vaccination rates between White and some BIPOC groups in the US – reflecting White Republican intransigence. While political factors have prevailed in the US, in the UK labour market factors predominate in the form of staff shortages in health and social care – these appear to have driven the move away from mandatory vaccination and have implications for public health and future pandemics.
While trade unions have played a key role in workplace health and safety during COVID-19 they walked a fine line between encouraging vaccination, opposing mandatory measures and supporting those who were reluctant to vaccinate. In both countries employers have introduced coercive measures by withdrawing sick pay for those who are unvaccinated – this may be considered pernicious when so many workers had inadequate access to these employment rights during the pandemic. A number of respondents explicitly linked the experience of frontline workers who worked throughout COVID-19 with vaccine hesitancy, particularly for those on non-standard contracts, often BME/BIPOC workers. The qualitative data would suggest that there is no positive relationship between risk of COVID-19 infection and frontline worker attitudes toward the vaccine, because of their exposure. One Oxford care worker described herself and colleagues as "walking weapons". Access to sick pay and leave is crucial to the disclosure of infection and prevention of COVID-19 transmission in the workplace. The UK survey data indicates that perceptions of economic risk are associated with negative frontline worker attitudes toward the vaccine. Positive experiences of health and safety in the workplace appear associated with more positive vaccine behaviour.
In both Manchester and Oxford, there were particular issues for migrant workers and refugees with insecure employment status and fears about documentation and registration. Across both cities legacies of racism informed the perceptions of BME/ BIPOC communities, fuelled by more recent experiences. At the same time, the focus of the study on frontline workers questions the racialisation of vaccine hesitancy, suggesting the role of existing and intersecting structural inequalities. Respondents provided examples of measures to address vaccine hesitancy that had proved effective in both cities, focussing on tackling "hard to reach services" rather than "hard to reach communities" and "informing" rather than "promoting". As one SEIU officer put it, open dialogue was necessary to address the"very valid vaccine hesitancy that comes from deep historical places in particular communities and to not override it or ignore it but actually talk about it directly." (USKI10)
References
Burns, C., Mearns, K., McGeorge, P. (2006). Explicit and implicit trust within safety culture. Risk Analysis, 26(5), 1139-1150; Reason, J. (1997). Managing the risks of organizational accidents. Ashgate.
Cai, M., Moore, S., Ball, C., Flynn, M. (2022) The role of Health and Safety Representatives in COVID-19: 22 February 2022.
Chaudhuri, K., Chakrabarti, A., Chandan, J.S. et al. (2022). COVID-19 vaccine hesitancy in the UK: a longitudinal household cross-sectional study. BMC Public Health 22, 104 (2022).
Dorling, D. (2021) Who are the unvaccinated and what is happening to them?: Retrieved 7 March 2022.
Freeman, D. et al. (2020) COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes and narratives survey (Oceans) II. Psychological Medicine, 1-15.
Frick, K. (2011). Worker influence on voluntary OHS management systems – A review of its ends and means. Safety Science, 49(7), 974-987.
Gollust SE, et al. (2018). What Causes Racial Health Care Disparities? A Mixed-Methods Study Reveals Variability in How Health Care Providers Perceive Causal Attributions. Inquiry. 2018 Jan-Dec;55:46958018762840.
Kata, A. (2012). Anti-vaccine activists, Web 2.0, and the postmodern paradigm – An overview of tactics and tropes used online by the anti-vaccination movement, Vaccine, 30(25), 3778-3789.
MacKenna B, Curtis HJ, Morton CE, et al. Trends, regional variation, and clinical characteristics of COVID-19 vaccine recipients: a retrospective cohort study in 23.4 million patients using OpenSAFELY.medRxiv 2021. [Preprint.] https://www.medrxiv.org/content/10.1101/2021.01.25.21250356
Martin CA, Marshall C, Patel P, et al. (2021) Association of demographic and occupational factors with SARS- CoV-2 vaccine uptake in a multi-ethnic UK healthcare workforce: a rapid real world analysis. MedRxiv [Preprint]. https://www.medrxiv.org/content/10.1101/2021.02.11.21251548v2
Mnookin, S. (2011). The Panic Virus: A True Story of Medicine, Science and Fear. Simon & Schuster.
Public Health England (2020) Beyond the Data: Understanding the Impact of COVID-19 on BAME Communities (publishing.service.gov.uk)
Runnymede Trust (2020), Over-Exposed and Under-Protected, The Devastating Impact of COVID-19 on Black and Minority Ethnic Communities in Great Britain, Release date: August 2020.
Razai M., Kankam, H., Majeed, A., Esmail, A. and Williams, D. (2021) Mitigating ethnic disparities in COVID-19 and beyond, BMJ 2021;372:m4921 https://doi.org/10.1136/bmj.m4921
Razai, M., Osama, T., McKechnie, G., Majeed, A. (2021) COVID-19 vaccine hesitancy among ethnic minority groups, BMJ 2021;372:n513 https://www.bmj.com/content/bmj/372/bmj.n513.full.pdf
SSHAP (2021) What can social science research teach us about COVID-19 vaccine deployment?: 15 September 2021.
Streefland P, Chowdhury AM, Ramos-Jimenez P. (1999). Patterns of vaccination acceptance. Soc Sci Med. 1999 Dec;49(12):1705-16.
Woolf, K. et al. (2021) Ethnic differences in SARS-CoV-2 vaccine hesitancy in United Kingdom healthcare workers: Results from the UK-REACH prospective nationwide cohort study, THE LANCET Regional Health Europe, 9, 100180, October 01, 2021.
Citations
- The term BME/BIPOC is used to cover the UK term Black and Minority Ethnic and the US term Black, Indigenous and People of Color.
- Ajzen, I. & Fishbein, M. (2005). The influence of attitudes on behaviour. In Albarracin, D.; Johnson, B.T.; Zanna M.P. (Eds.), The handbook of attitudes, Lawrence Erlbaum Associates.
- The Guardian (2021) Our key findings about US healthcare worker deaths in the pandemic’s first year, Release date: 8 April 2021.
- New Hampshire Charitable Foundation (2021) New Community Health Workers Will Help With COVID Response in Manchester, Release Date: 12 February 2021.
- Public Health England (2020) Beyond the Data: Understanding the Impact of COVID-19 on BAME Communities (publishing.service.gov.uk)
- Runnymede Trust (2020), Over-Exposed and Under-Protected, The Devastating Impact of COVID-19 on Black and Minority Ethnic Communities in Great Britain, Release date: August 2020.
- Oxford University Hospitals NHS Trust (2020), Varying risk of COVID-19 to health workers revealed, https://www.ouh.nhs.uk/news/article. aspx?id=1312, Release date 30 June 2020.
- Centers for Disease Control and Prevention (2022) COVID-19 Vaccinations in the United States, Release date: 28 February 2022.
- GOV.UK Coronavirus (COVID-19) in the UK (2022) Latest reported vaccination uptake, Release date: 28 February 2022.
- Centers for Disease Control and Prevention (2022) Demographic Trends of People Receiving COVID-19 Vaccinations in the United States, Release date: 28 February 2022.
- Office for National Statistics (2022) Coronavirus (COVID-19) latest insights: Vaccines, Release date: 28 February 2022.
- ibid
- Office for National Statistics (2022) Coronavirus (COVID-19) Infection Survey technical article: Analysis of characteristics associated with vaccination uptake, Release date: 15 November
- Razai M., Kankam, H., Majeed, A., Esmail, A. and Williams, D. (2021) Mitigating ethnic disparities in COVID-19 and beyond, BMJ 2021;372:m4921 https://doi.org/10.1136/bmj.m4921
- Razai, M., Osama, T., McKechnie, G., Majeed, A. (2021) COVID-19 vaccine hesitancy among ethnic minority groups, BMJ 2021;372:n513 https://www.bmj.com/content/bmj/372/bmj.n513.full.pdf
- SHRM (2021) Health Care Worker Vaccination Deadlines Extended in Some States, Release Date: 21 January 2022.
- BMJ 2021;374:n2238 COVID-19: US imposes mandatory vaccination on two thirds of workforce, Release Date: 13 September 2021.
- BMJ 2022;376:o269 COVID-19: Government abandons mandatory vaccination of NHS staff, Release Date: 01 February 2022.
- Nursing Times (2022) Former CNO backs calls to delay mandatory COVID-19 vaccines, Release Date: 21 January 2022.
- The New York Times (2022) Who’s Requiring Workers to Be Vaccinated?, Release Date: 23 February 2022.
- NBC News (2022) From Amex to Walmart, here are the companies mandating the Covid vaccines for employees, Release Date: 25 January 2022.
- People Management (2022) Can employers reduce sick pay for unvaccinated staff?, Release Date: 11 January 2022.
- The Conversation (2021) Why so many unions oppose vaccine mandates – even when they actually support them, Release Date: 9 November 2021.
Summary
- Published
© The authors. This is an open access publication licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 Unported License
To cite this report: British Academy (2022), Understanding Vaccine Hesitancy Amongst Frontline Workers: The influence of trade union and community representatives, The British Academy, London
- DOI doi.org/10.5871/c19-recovery/S-M-C-B-N-C-CC-W-M-E-A (Opens in a new window)