The COVID-19 YPAR Project
Youth Participatory Action Research (YPAR) to explore the context of ethnic minority youth responses to COVID-19 vaccines in the United States and United Kingdom
By Megan Schmidt-Sane, Tabitha Hrynick, Elizabeth Benninger, Janet McGrath, Santiago Ripoll, Brinda Athreya and Jillian Schulte
Download PDF report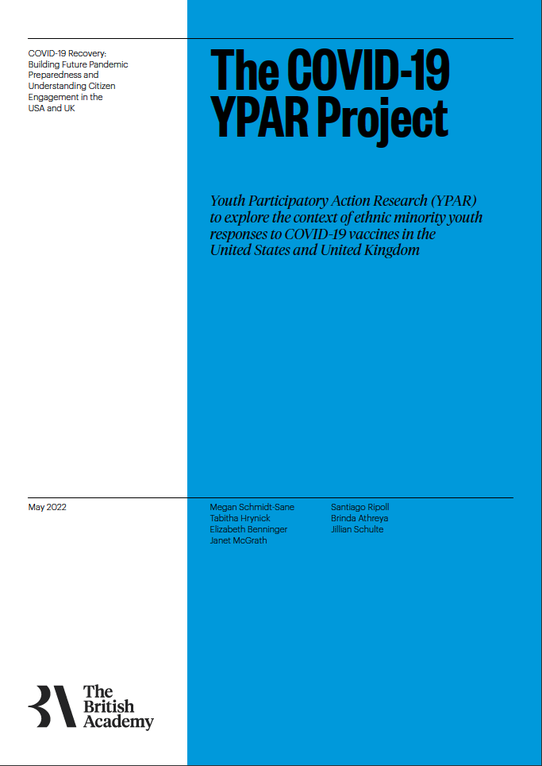
- Published by
- British Academy
- Year
- 2022
- Pages
- 34
About the authors
Dr Megan Schmidt-Sane is a Postdoctoral Researcher at the Institute of Development Studies. Tabitha Hrynick is a Research Officer at the Institute of Development Studies. Professor Elizabeth Benninger is a Professor of Psychology at Cleveland State University. Dr Santiago Ripoll is a Research Fellow at the Institute of Development Studies. Professor Janet McGrath is the Chair of Anthropology and Associate Professor of International Health at Case Western Reserve University. Dr Brinda Athreya is a Qualitative Research Associate at Case Western Reserve University. Dr Jillian Schulte is a Graduate Research Assistant at Case Western Reserve University.
About the COVID-19 Recovery: Building Future Pandemic Preparedness and Understanding Citizen Engagement in the USA and UK
The programme is the result of a partnership between the British Academy, the Social Sciences Research Council (SSRC) and the Science & Innovation Network in the USA (SIN USA) to award funding to ten transatlantic studies focusing on UK-US COVID-19 vaccine engagement. It follows a pilot study exploring levels of vaccine engagement in four locations across the US and UK, while the larger programme was expanded to study multiple locations. The programme was funded by the UK’s Department for Business, Energy and Industrial Strategy.
Executive summary
Despite progress in COVID-19 vaccination rates overall in the US and UK, vaccine inequity persists as young people from minoritised and/or deprived communities are often less likely to be vaccinated. COVID-19 ‘vaccine hesitancy’ is not just an issue of misinformation or lack of information. ‘Vaccine hesitancy’ among young people is reflective of wider issues such as mistrust in the state or the medical establishment and negative experiences during the pandemic.
This report is based on case study research conducted among young people (ages 12-18) in Cleveland, Ohio, US and the London borough of Ealing, UK. Whilst public discourse may label young people as ‘vaccine hesitant,’ we found that there were differences based on social location and place and this labelling may portray young people as ‘ignorant.’ We found the greatest vaccine hesitancy among older youth (15+ years old), particularly those from minoritised and deprived communities.
Unvaccinated youth were also more likely to be from families and friend groups that were unvaccinated. While some expressed distrust of the vaccines, others reported that COVID-19 prevention was not a priority in their lives, but instead concerns over food security, livelihood, and education take precedence. Minoritised youth were more likely to report negative experiences with authorities, including teachers at their schools and police in their communities.
Our findings demonstrate that COVID-19 vaccine hesitancy is embedded in a context that drives relationships of mistrust between minoritised and deprived communities and the state, with implications for COVID-19 vaccine uptake. Young people’s attitudes toward vaccines are further patterned by experiences within their community, school, family, and friend groups.
Key Findings
- Not all young people are COVID-19 vaccine hesitant, but instead vaccination uptake is patterned by age, community experiences of marginalisation and deprivation, and family and peer influence.
- Unvaccinated youth were more likely to be older, and from more deprived communities.
- Youth report having access to a lot of information on COVID-19 vaccines, though misinformation dominated social media when vaccines first came out.
- Younger youth were more likely to be vaccinated and have family members and friends who were vaccinated.
- Youth, particularly from deprived areas, face numerous challenges, some related to the pandemic. Young people reported experiences of racism in schools and through interactions with police. This may contribute to a sense of mistrust in the ‘system.’
- Young people across contexts reported symptoms of depression and anxiety during the pandemic, which contributed to a lower sense of well-being.
- Unvaccinated youth were more likely to feel unsupported in their lives, have fewer opportunities, and rely on youth centres as ‘safe spaces,’
This report is structured as follows. Annexes are available which include 1) a full- length case study of Cleveland, 2) a Cleveland-focused policy brief on vaccine hesitancy, 3) a full-length case study of Ealing, and 4) an Ealing-focused policy brief on vaccine engagement.
- Section 1.0 includes an introduction and reviews key concepts, terms, and definitions that are at the centre of this research.
- Section 2.0 briefly reviews the literature on youth in relation to vaccine hesitancy, a political economy of health framework, systemic racism and structural inequalities, and trust and mistrust in authorities.
- Section 3.0 presents the comparative case study findings.
- Section 4.0 details policy recommendations for Cleveland and Ealing public health actors, with relevance to a wider range of local and national policymakers in the United States and United Kingdom
Introduction
Young people from minoritised communities in the urban UK and US often feel ignored when it comes to COVID-19 policies, including vaccination efforts. This research shows how histories of neglect – including racialised policies – and youth experiences of deprivation contribute to lower COVID-19 vaccination uptake.
While many young people reported acceptance of the COVID-19 vaccines, those from deprived communities disproportionately report rejecting vaccination. Young people linked this rejection to COVID-19 being less of a pressing concern, mistrust in authorities rooted in a lack of state support for young people’s needs, and perceived inadequate funding for youth services. Despite progress, young people from deprived areas face deeply rooted obstacles to COVID-19 vaccination. What this report will show is that COVID-19 vaccination is representative of more deeply ingrained relationships of mistrust between young people and authorities in the US and UK. Without urgent action, young people may continue to feel disengaged with ripple effects across society.
Vaccine hesitancy is embedded in social and political-economic context
Recent studies have shown how minoritised communities often have a deeper mistrust of the medical establishment and government, due to long histories of medical experimentation, neglect, and systemic racism. This history shapes young people’s attitudes toward vaccination in differing ways, often depending on their socioeconomic status. Emerging literature found that medical mistrust was associated with social isolation, financial insecurity, socioeconomic status, and level of social support.(1) Research on youth vaccination attitudes also has shown that youth ‘vaccine hesitancy’ may be linked to youth willingness to get vaccinated in light of peer and parental views(2) and social media.(3)
To identify the context of youth vaccine attitudes, we conducted case study research in Cleveland, Ohio in the United States and the London borough of Ealing in the United Kingdom using traditional and participatory methods. We led in-depth interviews and focus group discussions with 123 young people (ages 12-18) largely from minoritised communities, while youth advisory boards provided oversight and input into the research. We also conducted a political-economic analysis of each place to understand how structural inequalities might underpin vaccine attitudes and to answer our guiding research questions. These included:
1) How does context specific to social location (ethnic minority youth) and physical place (disadvantaged neighbourhoods), including experiences of systemic racism, structural inequalities, and historical injustice shape responses to COVID-19 vaccines?
2) How do youth conceptualise (mis)trust and what might be the role of (mis)trust in youth responses to COVID-19 vaccines?
This short report shares findings from the research with an aim to inform policy responses by decision-makers in the UK and US working on youth COVID-19 vaccine engagement.
Key concepts, terms, and definitions
Political economy of health considers the historical, political, and economic contexts in which disease and illness arise, and examines the ways in which societal structures interact with place conditions that lead to good or ill health.
Systemic racism is a socially constructed scaffolding that supports and maintains racial discrimination and while racism may shift over time, the scaffolding continues to hold it in place.
Structural inequalities result from and intersect with various -isms (e.g. racism, sexism etc.) and are deeply embedded in our societies. Structural inequalities include two key components; persistence where inequalities are reinforced and compounded over time and intersectionality where relationships between inequalities shape different experiences for individuals facing multiple forms of oppression.
Place conditions refer to a community’s historical, social, and political-economic context.
Trust, specifically medical mistrust, refers to a tendency to distrust medical systems and personnel believed to represent the dominant culture in a given society. Distrust in the broader COVID-19 response, a lack of trust in political authorities, and/or distrust in broader institutions have been cited in a broad range of ethnic minority responses to COVID-19 vaccines and other measures.
Vaccine hesitancy refers to a delay in acceptance or total refusal of vaccines despite the availability of vaccination services.
Vaccine confidence is the belief that vaccination, and the providers, private sector, and political actors behind it, serve the public’s best health interests.
Vaccine equity is fair and just access to vaccines, prioritizing historically marginalised and disadvantaged communities. The most effective way to achieve equity is by involving communities in the planning, execution, and decision-making process of COVID-19 vaccination programmes and by addressing histories of racism, injustice, and oppression.
Racialised and ethnic minorities include groups that have been minoritised over time on the bases of ethnicity. In the United States, Black, Indigenous, people of colour (BIPOC) is a unifying label that also emphasises the unique experiences of Black and Indigenous communities. In the context of this report, we write separately about Black (American), Latine/Latinx, and Asian (South Asian, Southeast Asian, East Asian) communities. In the United Kingdom (in the context of Ealing), we write about Black African, Black Caribbean, and South Asian communities. In the aggregate, we may describe these groups as racialised communities, ethnic minorities, or BIPOC, although in the UK, the term Black and Minority Ethnic, or BAME, is commonly used.
Background
This section includes an overview of vaccine hesitancy and the structural forces that shape relationships between young people, the communities in which they live, and local and national government. This provides us with a better understanding of how place conditions shape youth responses to COVID-19 vaccines and embeds individual attitudes of hesitancy or confidence in a wider ecosystem.
Box 1. Engaging with young people in a pandemic
While older adults were generally more vulnerable to COVID-19, young people were largely more vulnerable to the psychosocial and economic impacts of COVID-19 measures, especially stay-at-home orders or ‘lockdowns.’ Youth experienced unique challenges during the COVID-19 pandemic including school closures and months of online class, social isolation, mental health issues, and loss of services and support. Many young people now experience great uncertainty about the future, rooted in this disruption of their education and career path. This uncertainty is also driven by a scepticism that adult authorities, from government to the medical establishment, can fix these interlocking crises. Encouraging vaccination uptake requires trust. Building trust with young people, particularly from racialised and disadvantaged communities, will require novel strategies, shifts toward understanding trust as a community construct, rather than an individual one, and deep engagement. As such, vaccination programs designed for adults will not necessarily work for youth
Youth vaccine hesitancy
The World Health Organization defines vaccine hesitancy as a ‘delay in acceptance or refusal of vaccines despite the availability of vaccination services.’(4) It is not a dichotomy of being ‘hesitant or not,’ but rather a continuum ranging from complete acceptance to complete refusal.(5) As social scientists have noted,(6) the term ‘vaccine hesitancy’ can sometimes ignore a wide spectrum of responses and attitudes toward COVID-19 vaccines. ‘Vaccine hesitancy’ labelling often may mask historical neglect and oppression that contributes to a ruptured relationship between communities and the state, and communities and the medical establishment.(7)
Social scientists have long drawn attention to the need to understand vaccine hesitancy in context.(8) Ethnic minorities, including Black, Black African and Caribbean, Asian and Latine/Latinx youth have experienced histories of systemic racism in the UK and US, and particular histories related to policing and immigration which compound experiences of injustice. Childhood exposure to traumatic events stemming from racism, xenophobia, and discrimination are acknowledged major life stressors.(9) In both the UK and US, race intersects with gender, social class, and other identity categories to shape experiences.
In both the US and UK, policy discussions around COVID-19 vaccine hesitancy are intertwined with discussions of racism and injustice, poverty, and deprivation, and being in a younger age group.(10) Some of these narratives gloss over differences and some link vaccine hesitancy to ‘less scientific knowledge,’ which could, for example, perpetuate harmful stereotypes about minoritised communities.(11)
Few studies have looked explicitly at systemic racism and even fewer at how youth experiences throughout the life course, including during the pandemic, might shape their responses to the COVID-19 vaccine. There is value in research that links young people’s perceptions and responses to vaccines to the place conditions in which they live.
Box 2. Youth vaccine attitudes
Vaccine attitudes among youth differ from adults in several important ways. First, in some contexts, young people cannot make the decision to get vaccinated on their own, they may require parent permission. Second, young people are embedded in school contexts where historically they have received other kinds of health information. Third, young people may be subject to specific vaccine mandates related to participation in school sports or other related activities. Lastly, young people may face higher levels of social and peer pressure to get vaccinated, or not.
In the UK, if someone is under the age of 16, parental consent will be sought for COVID-19 vaccinations. However, children can consent themselves, without parents, if they are deemed competent or what is called ‘Gillick-competent.’ Medical professionals have received training about how to ascertain whether someone has the competence to consent. In practice, some medical professionals are hesitant to apply the Gillick-competent standard for COVID-19 vaccinations.
In the US, each state has its own consent laws, ranging from required parental consent for COVID-19 vaccination to children as young as 11 years old allowed to get vaccinated without parental consent. In Ohio, parental consent is required for anyone under the age of 18.
Systemic racism and structural inequalities underpin vaccine attitudes
Longstanding systemic racism and structural inequalities on both sides of the Atlantic play a fundamental role in the differential impact of COVID-19, attitudes toward vaccines, and the interpretation of and trustworthiness of vaccine messages and messengers.(12) Systemic institutional racism is a socially-constructed scaffolding that supports and maintains racial discrimination and while racism may shift over time, the scaffolding continues to hold it in place.(13) This scaffolding is supported by intersecting -isms: colonialism, sexism, xenophobia, nativism, capitalism, and class structures which have historically assisted in the development of the UK and the US. There are also differences between the UK and US contexts, including different health systems (centralised/decentralised) and community contexts, which shape the impact of structural disadvantage and experiences of the COVID-19 pandemic.
Structural inequalities result from and intersect with various -isms and are deeply embedded in our societies. Structural inequalities include two key components.
- Persistence where inequalities are reinforced and compounded over time and
- Intersectionality where relationships between inequalities shape different experiences for individuals facing multiple forms of oppression.(14)
Crenshaw’s intersectionality theory is key to understanding how race, class, gender, immigration status, and other identities intersect to shape an individual’s life experience based on their multiple identities and social positions.
Despite these persistent forces of oppression, life experiences of systemic racism and structural inequality are often left out, acontextualised, or assumed to have homogenous effects on minoritised communities’ perceptions of COVID-19 vaccines.(15) As an extension of understanding patterns amongst minoritised youth, more must be done to untangle the pathways between experiences of injustice, experiences of social location, and responses to COVID-19 vaccines amongst youth. Public health discourse around ethnic minorities often focuses on discrete impactful events in the historical record rather than the everyday experiences of racism and inequalities which in turn shape relationships of mistrust between ethnic minorities and authorities.
Trust and mistrust in authorities
Box 3. Medical mistrust
Medical mistrust means a tendency to distrust medical systems and personnel believed to represent the dominant culture in a given society. The interpretation that medical mistrust is solely due to the Tuskegee Syphilis Study neglects longstanding historical injustice that occurred prior to that experiment and has continued since (i.e. medical experimentation on slaves, exploitation after the Civil War, etc.). It also ignores the similarities in cross-contextual findings on trust, and how US historical events might shape minoritised youth’s mistrust in the UK, as well as ongoing negative experiences of health services that many BIPOC continue to face.
The role of trust is a cornerstone of the relationship between communities, public health, and other government actors.(16) Trust affects the reception, interpretation, and spread of health communication on COVID-19 measures and vaccines. While loss of trust has been documented as a ‘key determinant’ in vaccine hesitancy, trust is often conceptualised as static (e.g., trust can be built once). Understanding responses toward COVID-19 vaccines would require a more dynamic understanding of how trust is constructed, (re)negotiated, and contextualised particularly for ethnic minority youth embedded in intersecting histories of inequality, racism, oppression, and injustice.
Experiences of injustice are widely viewed to affect trust and COVID-19 vaccine confidence.(17) Medical mistrust and mistrust in authorities seem to mediate experiences of racism and inequalities and how this affects responses to COVID-19 vaccines. Trust is frequently mentioned in the literature on vaccines,(18) although less is known about how trust is experienced, conceptualised, deployed, and (re)built.
Amongst adults, medical mistrust is linked to broader experiences with authorities that have ruptured relationships of trust with minoritised communities. Research with adults has shown that COVID-19 vaccine hesitancy among Black adults was not only due to high medical mistrust, but this was underpinned by a lack of policy and political responses to the Black Lives Matter movement’s priorities for change.(19) Further, police brutality that was experienced personally or through media reports also increased medical mistrust.(20)
There are very few studies that have specifically examined medical mistrust amongst youth in the context of health research.(21) However, ‘youth mistrust’ in government is frequently cited in discourse around low uptake of COVID-19 vaccination. Ash and colleagues (2021) found that social isolation, financial insecurity (e.g., job loss, loss of income) due to the COVID-19 pandemic, and eligibility for free or reduced lunch predicted medical mistrust.
A political economy of health approach to youth ‘vaccine hesitancy’
Several studies have focused on the historical, social, cultural, and political drivers of vaccine hesitancy,(22) though there are gaps in the evidence with regard to minoritised youth vaccine hesitancy. This study used a political economy of health approach to frame the experiences of young people in the US and UK and to understand how minoritised youth experiences, rooted in historical and political-economic context, can drive vaccine hesitancy today.
A political economy approach examines the structural determinants of health, which are fundamentally the ‘causes of the causes’(23) and our framework explicitly includes systemic racism as a key driver of inequalities. A political economy of health thus considers the political, social, cultural, and economic contexts in which disease and illness arise, and examines the ways in which societal structures interact with place conditions that lead to good or ill health.(24)
A political economy of health approach to youth vaccine hesitancy will keep the structural determinants of health (e.g., economic stability, neighbourhood environment, social and community context) and social justice at the centre of our understanding.(25) For minoritised youth, exploring the structural determinants of vaccine hesitancy will enable the design of engagement approaches that address ‘root causes’ rather than symptoms of vaccine hesitancy.
This approach widens our understanding of vaccine hesitancy beyond focusing on individual behaviour and motivations. It also recognises the fluidity between context and individual agency, where individual agency still plays a role and structures are not overly deterministic. It focuses our attention on how historical and unequal economic arrangements and high burdens of chronic diseases intersect as power differentials within the provision of healthcare,(26) enabling a more comprehensive assessment of the context of COVID-19 vaccination and youth responses to vaccines.
Political economy also brings attention to the erosion of government investment in youth opportunities. Young people, particularly from deprived areas, are increasingly marginalised while being framed as ‘trouble’ or in need of disciplining. Finally, a political economy of health framework helps to explain the role that systemic racism and structural inequalities play in structuring minoritised community experiences, shaping relationships between minoritised communities and authorities, and how relationships of trust drive (or hinder) youth uptake of COVID-19 vaccination.
Figure 1. Conceptual framework for the ‘Political Economy of Youth COVID-19 Vaccine Hesitancy’
Our conceptual framework (Figure 1) uses political economy of health to frame youth vaccine hesitancy. Our report will demonstrate how young people’s views on vaccination are underpinned by the following key factors:
- Systemic racism and structural inequalities. Longstanding experiences of systemic racism drive inequalities between majority and minority communities. Young people from minoritised backgrounds and living in deprived areas are less likely to have positive experiences with government authorities, especially police. This may lead to greater mistrust in the ‘system.’
- Austerity. The US and UK governments have reduced funding for essential government services like youth services, youth centres, and recreation centres. This reduced funding disproportionately affects vulnerable youth. In the UK, austerity policies have led to a deficit of funding available for local governments and youth services are on the decline in many places.
- Community experiences. For racialised minorities, in addition to community experiences of deprivation, young people are often labelled as ‘dangerous,’ or ‘anti- social,’ and experience police surveillance through frequent stops and searches. In this report, we will show how these trends underlie youth marginalisation and lower vaccine uptake, with implications for future public health engagement with youth on COVID-19 vaccination and beyond.
- School environment. Youth receive information, including information about health, in schools. Science-focused education and education about how vaccines work can shape youth attitudes toward COVID-19 vaccines.
- Family influence. Many youth cannot decide whether to get a vaccine, as this may depend on parental decisions. Even when they can decide however, family attitudes may also influence them and conversely, young people reported influencing parental vaccination decisions.
- Peer influence. Young people are more likely to be vaccinated if their peers are vaccinated, as social and peer influence is critical in adolescence and teenage years.
Research overview and findings
Research approach
The findings presented here are based on Youth Participatory Action Research (YPAR) and a comparative case study approach to research on young people’s (ages 12-18) COVID-19 vaccine responses in Cleveland, Ohio and Ealing, London. We used a political economy of health analysis to provide contextual depth to each case study and to explore the historical roots of systemic racism and structural inequalitiesin each place. We used a comparative case study approach(27) to generate more generalisable insights across our two cases. The comparative case study approach allows us to bring these different methods together to understand, in-depth, the background to ethnic minority youth’s responses to COVID-19 vaccination.
This research was conducted over a five-month period, from November 2021 to March 2022. We also used a Youth Participatory Action Research (YPAR) approach which explicitly aims to increase youth participation in research and social change.
Box 4. Cleveland case study: Political-economic context
Cleveland’s long and complicated history of racial diversity, marked by discriminatory housing policies (‘redlining’) and segregation in schools, among other injustices, shapes how the city’s Black youth relates to and trusts in authorities and what kinds of opportunities are available. Cleveland, Ohio is a key feature of the ‘Rust Belt,’ which comes from its long history in the steel industry.
The city is somewhat geographically divided between a west and east side, with the Cuyahoga River running between. In Cleveland, as in many other cities, place matters. Where you live in the city determines what kind of housing quality is available, which schools children can go to, and whether there are supermarkets with healthy foods to purchase.
Patterns of racial inequities show up in wide health and education disparities, as Black populations face higher infant mortality, Black and Latine/Latinx are 3 times more likely to live in poverty (compared to whites) and Black Clevelanders have a life expectancy that is 6 years lower than whites. These inequities have longstanding historical roots.
Experiences of BIPOC youth in Cleveland mirror many faultlines in the United States. In Cleveland, narratives of BIPOC youth are racially driven and over-emphasize stereotypes of youth involvement in local gangs, and community violence, including gun violence. BIPOC youth are, however, disproportionately represented in the justice system. While disparities have improved in recent years, there are still significant disparities in the justice system. In 2018, Black youth accounted for 56% of incarcerated youth in Ohio despite representing just 16% of under-18s in the state.
While Cleveland has longstanding racial inequities, the city has undergone a period of growth and ‘revitalization,’ though this has not been equitably distributed. The city has seen both neoliberal urban regeneration plans and community development schemes, but this has not fixed persistent socio-spatial inequalities. These schemes have emerged as a part of the ‘logics and politics’ of post-2007 austerity urbanism. Local political coalitions have promoted demolition of abandoned or foreclosed homes, as a part of this revitalization, though in reality this has just cleared the way for privatised reinvestment and luxury apartment buildings, many of which remain out of reach of Cleveland’s poorer residents.
Box 5. Ealing case study: Political-economic context
The London Borough of Ealing, in west London, is the third largest borough in the city and one of the most ethnically diverse areas of the United Kingdom. Ealing is home to about 352,000 residents, nearly half of whom were born abroad in over 170 different countries. This number is also thought to be an undercount, due to the large number of undocumented immigrants residing in the borough. Due to this rich mix of people, Ealing is one of the UK’s most diverse local authorities.
The Ealing Race Equality Commission was set up in late 2020 by the Council to examine race inequality in detail in the borough, including how structural and racial inequalities shape outcomes across the life course. In their recently published report, they focused on five themes including education and learning; income and employment; crime and justice; participation; decision-making and leadership; and health and housing. The commission highlighted that while there has been a long tradition of anti-racist activism in the borough, people in Ealing from minoritised backgrounds still face systemic disadvantages.
Many residents of Ealing also face economic precarity and poverty, including in-work poverty. Overall, the borough ranks 87th most deprived of 326 local authorities in England, according to the Index of Multiple Deprivation (IMD). The IMD is an official measure used in England taking into account income, employment, education, skills and training, health and disability, crime, barriers to housing service and living environment.
Austerity policies at the national level over several decades have restrained the budgets of local authorities which has made life yet more difficult for many in Ealing and across the UK as this has resulted in cuts to local social programs and serviceswe evaluate the evidence of austerity’s impact on health, through two main mechanisms: a ‘social risk effect’ of increasing unemployment, poverty, homelessness and other socio-economic risk factors (indirect. The Greater London Authority estimates that London boroughs may have seen a 63% reduction in real terms to their core funding over the last decade. In the context of Ealing, this has at times included funding for youth-oriented programs.
Key findings from our data
Youth vaccine hesitancy is based on place conditions and social environment
In our study, we heard a range of young people’s responses to COVID-19 vaccination. Differences in vaccine uptake mapped onto two different variables: age and socioeconomic status of the young person’s community. Younger participants largely had higher rates of vaccine uptake across contexts. Participants from communities with experiences of deprivation and racism were less likely to be vaccinated.
Young people reported that they do not necessarily lack good vaccine information, but rather that they are overwhelmed with information overall and much of it is misinformation. Promoting digital and news literacy among youth could be one part of mitigating vaccine hesitancy.(28)
Many are inundated with vaccine information from a plurality of sources, from news reports, to parental advice, to stories or anecdotes shared on social media sites like Instagram and TikTok.
Younger youth are less likely to be vaccine hesitant
In this study we found that acceptance differed by age across contexts, with younger participants (ages 12-14) being much more likely to be vaccinated compared to older participants (ages 15 and older).
These age-related differences are related to social context, as younger participants also discussed how their parents are influential in their thinking and how they receive vaccine information from their parents.
Younger participants, especially in the Cleveland context, were less likely to have access to smart phones and therefore were likely not as exposed to vaccine misinformation on social media compared to older youth. Younger youth in this study, particularly in Cleveland, were more likely to listen to their parents who had told them to get vaccinated and made sure it would happen. We know from existing literature on parent decision- making that some parents rely on community social norms to make their vaccination decisions.(29)
I got to two doses, and I got the booster like, like few days ago… Yeah, everyone [in my family is] vaccinated. My brother’s only got the two doses though, because the boosters are available to him, but everyone in the family is vaccinated… all my friends also vaccinated, I don’t know when they’re going to get the booster but they said they’re gonna get it.
–Male, South Asian (Indian), 12 years old, Cleveland
Vaccination to ‘return to normal’
Younger participants in this study, particularly in the US, spoke about the vaccine as a way to ‘return to normal,’ because it enabled them to attend more events, play sports, and visit friends’ houses without worrying too much about COVID-19. For instance, young participants in Cleveland spoke about needing to be vaccinated to attend friends’ birthday parties and other social events, which allowed them to feel socially connected and more ‘normal’ again.
In Ealing, participants reported that the hardest times were during lockdown. It is likely that there has already been some sense of returning to normal after lockdowns earlier in the pandemic. Additionally, for those individuals who did not ever prioritise COVID-19 prevention or could not be restricted due to needing to work, a ‘return to normal’ would look very different and may not be relevant at all. Because of this, there may be less incentive to get vaccinated to ‘return to normal.’
For older youth, the ‘return to normal’ had happened much earlier, as they likely had more autonomy (by virtue of being older) to visit friends and were more connected to others through social media and their phone. Older youth in both case studies were also working during the pandemic and were outside of the house. Those in Cleveland described their in-person work as something that saved them during the pandemic, because it allowed them to get out of the house and interact with others. Therefore, ‘returning to normal’ may not be as applicable or as much of an incentive for older youth to get vaccinated.
Older teens in Greenford, a less deprived area in Ealing, were largely vaccinated compared to their counterparts in the more deprived South Acton. In Greenford, older youth spoke about the importance of ‘following the science,’ and spoke negatively about their anti-vaccination peers who they thought were perhaps listening to conspiracy theories over scientific guidance.
Young people want to be safe, but ‘safety’ has different interpretations
In South Acton, similar to the older youth in Cleveland, concerns over safety dominated vaccine response narratives. This points to the importance of social location and place conditions in shaping how youth experience relationships with authority, and how that in turn affected their narratives on COVID-19 vaccination.
‘Safety’ was a recurring term that was interpreted differently by different age groups. In Cleveland, for example, younger youth spoke about vaccination as a way to be safe, to protect themselves and family members, and to maintain health and well-being.
For older youth, being ‘safe’ meant also doing what was best for their health, and that was to avoid what was perceived to be a risky or unsafe vaccine. This could point to one area of possible intervention, where notions of safety are discussed and validated, safety concerns are honestly acknowledged, and young people are given a chance to ask questions about vaccines.
I am too scared to get it. I don’t even necessarily know what’s in it because they could see what’s in it, but not give you the full story or just give it really scientific words to cover up something. So, I’m really just scared to get it. Yeah, my mom’s got it, but she hasn’t really felt anything but my dad had a really bad reaction to it. He was in hospital for a while.
Female, South Asian, 16 years old, Ealing
Experiences of deprivation may drive vaccine hesitancy
Box 6. Reasons cited for COVID-19 vaccine refusal
These are the range of reasons cited in our research for youth not getting COVID-19 vaccinated:
- Concerns over safety of the vaccines, particularly in the long-term
- Concerns over fast development of the vaccines and lack of testing
- Concerns over family members or others they knew who had died or gotten sick after getting vaccinated
- Disinterest or lack of relevance to their lives
- Perception that they were strong and healthy
- Perception that they could develop natural immunity without vaccination
- Perception that the government was forcing them to get vaccinated
Young people from minoritised backgrounds living in deprived communities were more likely to be vaccine hesitant. Vaccine hesitancy mapped onto local geographies, with youth in the more resourced area of Greenford expressing very different experiences compared to youth in the more deprived areas of South Acton and Northolt. This showed up in how young people in deprived areas experienced the pandemic in relation to other ongoing challenges, and this may have created a less conducive environment for taking up COVID-19 vaccines.
I just wish I don’t know I wish I had an answer. I wish I had one opinion, there’s so many points of views and perspectives and angles to look at this, there’s so many different parts of it that you have to think about, and consider before even trying to formulate a sentence about it that, I don’t know, I really, I do. I just wish that it was over.
Female, Mixed (White & Black), 18
In terms of vaccine refusal, we heard stories of young people who felt that the vaccines were unsafe and that it was best just to not get it. We heard more stories related to uncertainty than to certainty over the vaccine. Many who are ‘vaccine hesitant’ are inundated with information, unlikely to know which information to trust, less likely to have a parent convincing them to get vaccinated or to be vaccinated, and less likely to have friends who are vaccinated. This creates an information and social ecosystem whereby young people are less exposed to positive vaccine information and stories or anecdotes. Existing literature on COVID-19 vaccine hesitancy shows that knowing others or having ‘social norms’ related to vaccination are key to overcoming hesitancy.(30)
For young people in South Acton, for example, almost everyone was unvaccinated except for those who needed the vaccine to travel to see family abroad. Participants not only spoke about their vaccination status, but how parents and friends were similarly unvaccinated. In one interesting case, a young person did not want the vaccine, but he told his parents to get vaccinated for their own safety. He was relying on natural immunity rather than a vaccine.
Young people’s in-group shaped vaccine attitudes
Vaccination may to some extent rely on in-group solidarity, or at least basing behaviours and actions on what others in your in-group are doing. An in-group is a group of people who identify with each other based on a variety of factors, like gender, social class, age, race/ethnicity, and neighbourhood. Most vaccinated interview participants suggested that most of their friends and family members were vaccinated while the same was true of most unvaccinated participants, who reported most of their friends and families were also unvaccinated – although it was not always explicitly articulated as a reason for individuals’ vaccine decisions.
Through our observations at the youth centre in South Acton for instance, in-group thinking or bias was common but not necessarily explicitly articulated. They had similar narratives of their day-to-day realities, in which many described being more in survival mode. In contrast, interviewed participants in less deprived Greenford, seemed more future-oriented, with more of their concerns focusing around school and academic struggles and success.
Vaccine narratives that emphasise future-oriented thinking may not resonate with youth who face everyday precarity. The more similar positionalities and challenges faced by youth in each local context may shape their experiences and thinking in similar ways, while aspects of ‘belongingness’ or solidarity with one another as fellow in-group members may also play a role in the social reproduction of vaccine attitudes.
Youth experiences of place conditions
Young people’s responses to COVID-19 vaccines do not exist in silo, instead they are embedded in multiple, interlocking influences, from family and peer influence to community and place. In our political economy analyses, we demonstrated how in the Cleveland context, minoritised youth living in historically redlined areas are more likely to experience socioeconomic deprivation and fewer opportunities. In Ealing, austerity policies have led to funding cuts for local governments and youth services, whereas youth services provide critical opportunities which at-risk youth fundamentally rely on. In both cases, in the absence of opportunity, young people living in poverty have to think about providing for their families, avoiding the police, and getting through a school system that they perceive values them less. The experiences of young, minoritised, socioeconomically deprived participants fundamentally shape how they relate to and respond to public health guidance on COVID-19 vaccines.
Structural inequalities shape youth experiences of disadvantage
Young people spoke about their experiences of the education system, housing, and police surveillance, particularly in deprived areas of Cleveland and Ealing.
In Cleveland, youth reported narratives that relate to Black Americans’ experiences in the medical system, which included histories of medical experimentation like Tuskegee. Young people here spoke about redlining and how it affects where you live and what opportunities you have in life. In Cleveland, unlike in the UK, a predominantly Black public school system has prioritised Black-centred education, with teachings about Black Lives Matter, social justice, and redlining. This could be why these narratives show up in young people’s interviews. However, speaking about those issues did not necessarily predict vaccination status, as several youth were still vaccinated despite discussing the relevance of medical experimentation to their communities.
In Ealing, young people reported that experiences of living on estates or in deprived areas like South Acton or Northolt shape young people’s experiences in the education system and with police surveillance. It is significant, because in terms of local authorities and government, young people tend to interact with an education system that they perceive to be racist and with police that they perceive to be taking advantage of their power by arbitrarily stopping and searching teenage boys in the area.
In England, this directly relates to discourses about youth as ‘troublemakers.’ Young people know this discourse and refute it, saying that if policymakers just spoke to them, they would know what is going on in their lives. As reported by an Ealing youth worker and matched by study findings, young people know about this discourse, and it contributes to their sense of social exclusion and marginalization. Being frequently portrayed as ‘bad’ in social discourse is sometimes mirrored in vaccination discourse around youth who are non-compliant. It is important to avoid stigmatised labelling of the unvaccinated as non-compliant as it risks further alienating those who lack trust in institutions and systems. More research is needed to understand any potential linkages between public discourse, youth perceptions and lived experience, and vaccination uptake.
So basically, I don’t know how to explain. Personally, they [the police] judge you straightaway on your image, how you present yourself. They don’t give you the option to talk or express yourself to them. For example, if I go walk in the flats, if I got my hoodie up, I’m walking like this, just me being me, honestly, generally I’m not doing nothing. They see me, they’ll come straight over, and sometime if they don’t have their camera on, oh my god, because now they have to wear a body camera. So if they don’t have that on, honestly, they don’t care, they tell you to ‘shut up,’ they’ll be rude to you, they can do whatever they want honestly.
Male, Lebanese, 19-years old, Ealing
Young people experienced serious mental health challenges across contexts
Many participants’ COVID-19 experience was characterised by stress, uncertainty, instability, and a lack of clarity over what might happen in the near future. Youth also described perceived anxieties over getting COVID-19 and passing it to vulnerable family members. Others had pre-existing mental health challenges that worsened during the pandemic. In contrast, in three cases in Cleveland and one in Ealing, participants reported their mental health having actually improved quite a lot. Older teens in the study reported more experiences with depression and anxiety than younger teens, and females reported more mental health challenges than our male participants. However, these gendered differences may mean that females are simply more comfortable talking about mental health, compared to male counterparts.
In Ealing, uncertainties related to school and lockdown, social isolation, and disruption to young people’s educational and career goals contributed to a sense that they did not have control over their lives and that their future plans were now unclear.
While lockdowns had a very negative impact on many youths, successive lockdowns became increasingly difficult due to isolation, with this taking a negative toll on mental health. This was compounded by the stress of being constantly at home, particularly for those who live with several other family members or in a small home. For some youth participants, the availability of support in their social environment was critical to being able to cope with mental health challenges.
And this was like, way before the pandemic, because it was just like, I was deemed as being lazy, and I’m not lazy, I was just like, very sad. And so like, it’s really hard to like, focus on schoolwork, and focus on everything else, when like, there’s these like, negative thoughts just going on in your brain that you kind of feel like, you can’t really do that stuff, or what does it matter if you do that stuff or not? Like, who cares, you know., sit there and listen, basically, you don’t really do much, or they let you sign off early and things like that.
Non-binary, 18 years old, Native American and Black, Cleveland
What are young people and their families most concerned about?
Across case studies, the data suggest that youth’s responses to COVID-19 vaccines derive from lived experience in their community, including experiences of structural inequalities, such as redlining and socioeconomic deprivation. For youth in deprived areas, daily concerns are passed onto youth by their parents and peer groups, which may relate more to everyday experiences of racism or socioeconomic deprivation.
Unvaccinated youth may not be as concerned about COVID-19 or may not perceive it as relevant to their lives. In deprived areas, communities may prioritise livelihood security and safety over concerns about COVID-19.
In this case, we can use something of a ‘proximity’ argument. Many parents of minoritised youth speak to their children about keeping safe, staying away from police, or acting in a certain way if they are stopped by police. These are very present and pressing concerns. Meanwhile, young people’s parents in more middle-class areas are having conversations about COVID-19, how to protect yourself, wearing a mask, and getting vaccinated.
Young people do not trust the national government, but may still be vaccinated
Box 7. Youth understandings of ‘trust’
Understanding how young people view, operationalise, and deploy trust requires an emic or insider definition. This allows young people to say what ‘trust’ means to them, in their own experience. Participants reported various definitions of trust in relation to COVID-19 vaccination. While it was difficult to define as an abstract or hypothetical construct, young people operationalized trust as something that is relational. They could trust someone if they ‘knew them,’ knew their intentions, and their behaviour toward others.
Young people felt that someone could be trusted if they were familiar, if they acted in a way that demonstrated good intentions, if they were honest and transparent, and reliable. Low trust in politicians at the national level was matched by less familiarity with local politicians and fewer opinions on local government. Most youth across research contexts did not trust government. In both Ealing and Cleveland, older teens tended to trust those they were most familiar with – their mothers and girlfriends or boyfriends. This did not translate into higher vaccine uptake, as several Cleveland participants recounted that their parents asked them to get vaccinated and they did not. Also in both sites, younger youth had trust in their parents and parents were a source of influence in getting vaccinated.
However, more research is needed to understand the experiences of trust in relation to vaccine hesitancy. Anthropological research on vaccination in global settings has disabused many of the idea that the general public is ‘ignorant’ or only in need of education to accept vaccination.(31) Vaccine decisions are often not linear, and a paradigm that frames ‘ignorant publics’ in need of information, which leads them to accept a vaccine, may not be applicable to those with longstanding relationships of mistrust with authorities and institutions. In addition to talking about trust, we draw on a notion of ‘intuition,’ or someone’s ‘gut feelings’ that may direct them to feel a certain way toward vaccination without a conscious, rational, decision-making process.
(Mis)trust in government, being left behind
What this study of youth vaccine hesitancy points to is that vaccine hesitancy is about more than vaccines, it is also about the institutions that vaccines represent. Vaccines have social lives, meaning they take on political-economic, and social context, as anthropologists have long shown.(32) Similarly, vaccine hesitancy is social.(33) It represents, as this study has shown, histories of mistrust and social exclusion.
Our findings demonstrate that youth feel socially excluded, particularly those youth living in deprived areas. As one Ealing youth worker’s own data showed, these feelings of social exclusion can have ripple effects in terms of mistrust in government, mistrust in authorities, and now, vaccine hesitancy.
Young people lack trust in institutions, in part due to the lack of investment in their futures. Young people in this study, particularly those who spent time in youth centres, described the value of the youth centre space to their lives. Participants from Northolt travelled over one hour each way to reach the youth centre because there was no comparable option where they lived. For participants in Action and South Acton, the youth centre was a safe space where they could go after school, after work, to meet their friends and find support from youth centre workers. Among our South Acton participants, the primary youth centre worker was described by several young men as a ‘father,’ or a second father figure, who provided support, skills training as needed, and life and career advice. They felt like they could speak to him and that he listened to their perspective, whereas they did not have that kind of support elsewhere.
I think it’s like, when like the government make decisions. They just don’t have young people in mind when they make those decisions. So, like, if anything I would like, recommend that they, I don’t know do like some sort of survey or something. If they genuinely cared about the experiences of young people, then they do like some sort of survey to actually find out what young people think and what they want, and that because no politician is going to be making laws about what young people want because they don’t know what young people want. But often like it’s useless anyway, because the politicians don’t care about young people. They don’t genuinely care about any people anyways, they just want you know, get elected next year.
Female, white, 16 years old, Ealing
Medical (mis)trust drives youth vaccine hesitancy
Medical trust, or trust in doctors, public health, and other medical providers, did map onto vaccine attitudes more than other forms of trust. This matches the literature on adults from minoritised communities that have longstanding reasons to not trust the medical establishment.(34) One study(35) has explicitly linked experiences of police brutality to higher levels of medical mistrust, compared to those with no negative police encounters. This may point to the notion that young people, when they have negative experiences with one kind of authority (police, school), may translate that to mistrust in others (medical providers). For younger youth in Cleveland and Greenford youth in Ealing, trust in health care providers led many to take the ‘scientific approach’ to vaccination, meaning that they were more likely to get vaccinated.
That did not necessarily translate to vaccine uptake among older youth in Cleveland who did trust their family doctor.
Hypothetical questions about trust may be difficult for young people, especially younger participants, to answer. Young people did offer more insights when asked who or what information they trust, and why. Of note, many did not trust social media as a source of vaccine information. For those who did take the vaccine, they saw information on social media and then would check that information with a credible source like the NHS or CDC. For those who were not vaccinated, while they did not necessarily trust social media information, they also did not have an alternative nor were they necessarily seeking out alternative sources. It was more a matter of exposure and quantity – unvaccinated youth were exposed to accounts of vaccine safety issues, family members or friends who had become sick or died after the vaccine, and similar accounts on social media. There was less interrogation of the underlying causes of those illness or death accounts, and more an acceptance of the idea that ‘they got vaccinated, and died.’
While trust, particularly medical trust, is still a vital concept to understand in vaccine hesitancy research, it must be placed in context and understood based on developmental stage. For young people, ideas of who they trust are still evolving. Younger youth may have less exposure to community experiences of racist policies like redlining, police brutality, or unfair discipline in the education system. Younger youth may be shielded from needing to work to provide for their families. The concept of trust is quite general and needs to be further unpacked. For many young people, trust is contextual, it is relational, and it may even be emotional. It is based more on an intuition, a ‘gut feeling,’ rather than a rational assessment of familiarity, transparency, honesty, and good intentions.
Community rather than individual-level trust, and ‘intuition’ or ‘gut feelings’
Trust plays out in unexpected ways in youth vaccine hesitancy. On the one hand, high levels of mistrust in government did not always lead to vaccine hesitancy, as these sentiments were pervasive among youth in this study. Medical mistrust was more predictive, though again, we may need to focus on ‘trust in the vaccine’ rather than these other constructs. Finally, trust may not necessarily be an individual construct, or may not be relevant to studies of youth vaccine hesitancy as an individual construct. Young people’s trust in the vaccine is embedded in a social world.(36)
Community trust may be a more relevant construct to study vaccine hesitancy among youth. Community (mis)Trust important for minoritised youth with strong connections to migrant communities, Black communities or other groups that have been historically oppressed and have experienced injustice over generations. These community experiences, and everyday lived experience of inequalities and racism, particularly for older youth, creates an environment in which authorities (writ large) are less likely to be trusted.(37) In these cases, it becomes easier to accept questions over safety. Indeed, based on historical experience, it is prudent to be cautious when accepting new or potentially unsafe medical technologies. Therefore, it is vital that we understand and deploy notions of youth (mis)trust as historically rooted, contextualised, and relational.
A focus on ‘intuition,’ or a ‘gut feeling,’ may capture the wider range of initial and lasting responses of youth to vaccination. The concept of trust, as we have shown, may be too general and needs to be further unpacked, including how it relates to community experiences of structural inequalities. Young people may relate their feelings of (mis)trust to whether people in their social groups trust authorities and institutions. As we have shown, many youths feel socially excluded. In the absence of institutions that support young people, young people may turn to other youth as sources of information. There may be some trust in the collective wisdom of those around you, and if others are unvaccinated, they may know something that you do not. In short, more research can be done to unpack the experiences of mistrust, and to explore alternative concepts like intuition or gut feelings and what role they play in vaccine hesitancy.
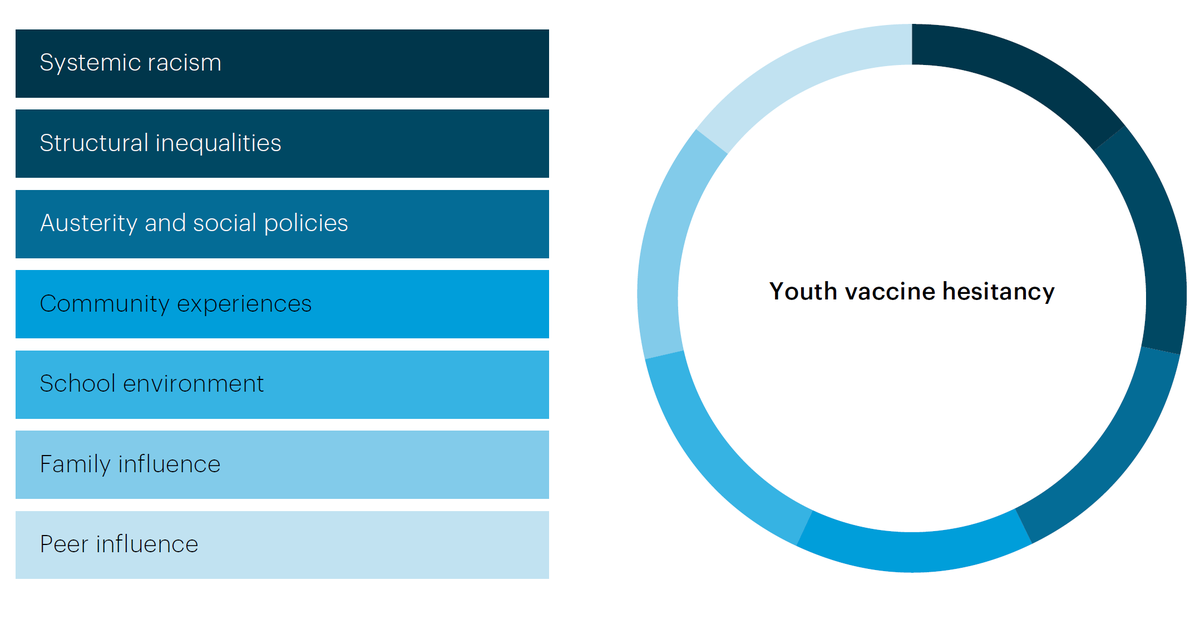
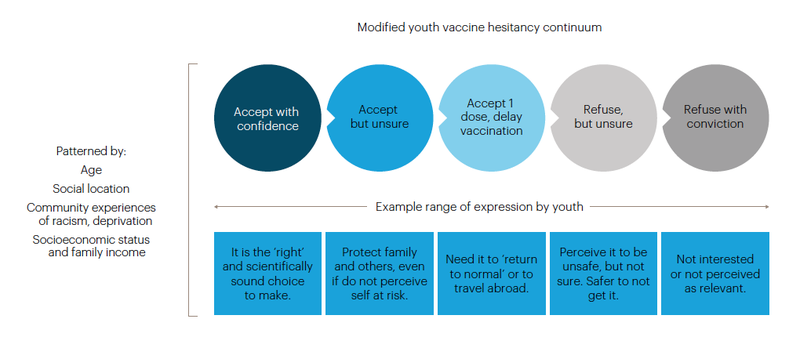
Youth vaccine hesitancy continuum
Based on these findings, we modified the 2014 SAGE Working Group of Vaccine Hesitancy framework. Figure 2 captures the range of youth COVID-19 vaccine hesitancies, ranging from total refusal to total acceptance, with a large number of people in-between in the ‘just not sure’ category.
Figure 2. Range of responses to COVID-19 vaccination, modified from the SAGE Working Group model (WHO, 2014)
Policy implications and future research
As we enter a more protracted phase of the COVID-19 pandemic, it is important to focus on people who have been ‘left behind,’ or less engaged in ensuring that they are equipped with information and access to services. Vaccine equity in Cleveland, Ohio and Ealing is critical as it will ensure that COVID-19 vulnerable communities have a high level of protection against COVID-19 disease and death. Vaccine equity points to the need for additional, tailored strategies that are responsive to, or embedded in, young people’s wider needs.
Improving COVID-19 vaccination among young people would necessitate strategies at various levels, ranging from the provision of information to changes in attitude and greater youth engagement within communities. Place of intervention include schools, youth spaces such as recreation centres, youth centres, or libraries, and with parents. Based on the available evidence, promising areas for intervention include:
National-level policymakers
- Consider ways to improve public awareness of COVID-19 vaccine safety. Given the speed at which COVID-19 vaccines were developed, it is important for national government to emphasise that no regulatory corners were cut and that vaccines were developed based on extensive prior research.
- Acknowledge public anxieties and uncertainty over COVID-19, including information about vaccines. Consider ways to enhance transparent and coherent public communication through consistent messaging. This should include acknowledgements of what we do not know or what we are not sure about.
- Work to build public trust and confidence in government services. Publics often trust governments that are able to deliver to citizens the services that they need, in ways that are equitable.(38) Endeavor to improve access to public services, quality and timeliness of public services, and respect for public service provision and citizens’ feedback.(39)
- Increase funding for local governments, including funds earmarked for youth services and opportunities. Providing young people with youth-friendly spaces can provide life-saving support that will enable them to flourish. Young people depend on youth services and fully supporting youth services will work to build trust between government and young people.
- Recognise that vaccination decision making is a complex and ongoing process rooted in young people’s political-economic and social experiences. It is not necessarily linear, in that someone will receive good vaccination information and act on it. For young people experiencing poverty, vaccination may not be a priority in their lives. Instead, engage with narratives that place vaccination within this context – of keeping young people safe in their risky work environments or at school, and how vaccination can help to ensure that they will not miss work due to lengthy illness.
Local public health officials
- Build more comprehensive and accessible social media campaigns to disseminate information to youth. Disseminate information through social media accounts like Instagram and Tik Tok, through locally well-known individuals.
- Train and engage youth peer leaders. Based on past work, peer leaders or vaccine champions could include young people from the communities that they would serve and who could engage with youth services and schools on vaccination.
- Consider shifting discourse around why young people should get vaccinated. Telling most young people to get vaccinated for their own health may not resonate with their experience of having a mild case of COVID-19, or the perceived idea that ‘natural immunity’ is a substitute for vaccination. Emphasise that young people should get vaccinated for their own health, to prevent symptoms associated with Long Covid, and to protect vulnerable family members.
- Disseminate information that young people over 16 do not need parental consent for vaccination in the UK. Some young people have the misconception that they need parental consent to get vaccinated. This is one potentially easy fix, to share information about the age of vaccine consent via news, schools/teachers, and social media.
- Work with other sectors, including youth services and non-profits, to create positive spaces for youth. While recreation centres and youth centres play a vital role in young people’s lives, there is a need for more youth-friendly spaces and for opportunities for young people to share their concerns and their voices. This may include space for young people to discuss experiences of other crises like mental health or policing practices.
- Provide support to mentors, teachers, and parents, to engage in positive conversations with young people about vaccination. This information could be tailored toward older teenagers, which we have found to potentially be more vaccine hesitant compared to younger peers. This could also include template lesson plans for teachers to teach news and media literacy skills, so that young people are equipped to discern between credible information and misinformation.
- Advocate with local government leaders for increased funding for, and engagement with youth services as a critical space in vulnerable youth’s lives. Youth services, including youth centres, are quite literally, life-saving services for young people. Many vulnerable young people in this study described how local youth workers were like a second parent to them and had connected them to vital services, like learning how to write a resume, or to job opportunities. These critical workers and youth centres must be better funded and supported.
Youth services
- Engage in listening sessions with youth to understand how remote schooling and disruptions to their education may impact how they relate to adult policy makers, including in public health. Young people were affected more by COVID-19 lockdowns or remote school than by the virus itself. If appropriate, consider using these sessions to answer questions about COVID-19 vaccination or refer youth to health services.
- Partner up with or start cross-sector mental health initiatives to respond to what may be an emerging crisis of anxiety, depression, and other mental health issues amongst youth. While many youths found critical help and their mental health improved during the pandemic, others express a lack of support. Working within schools and with community partners could be a critical aspect of supporting mental health.
- Facilitate dialogues between young people living in deprived areas and local police, on ‘neutral’ territory and with cross-sector involvement, including key community partners, youth workers, and parents. These dialogues could be a space for listening to young people’s experiences with police and identifying solutions to end harmful policing practices.
References
Alang, Sirry, Donna D. McAlpine, and Rachel Hardeman. ‘Police Brutality and Mistrust in Medical Institutions’. Journal of Racial and Ethnic Health Disparities 7, no. 4 (1 August 2020): 760–68. https://doi.org/10.1007/s40615- 020-00706-w.
Ash, Marcia J, Jannette Berkley-Patton, Kelsey Christensen, Regine Haardörfer, Melvin D Livingston, Teesha Miller, and Briana Woods-Jaeger. ‘Predictors of Medical Mistrust among Urban Youth of Color during the COVID-19 Pandemic’. Translational Behavioral Medicine, 3 June 2021, ibab061. https://doi.org/10.1093/tbm/ ibab061.
Bartlett, Lesley, and Frances Vavrus. Rethinking Case Study Research: A Comparative Approach. New York: Routledge, 2016. https://doi.org/10.4324/9781315674889.
Benkert, Ramona, Adolfo Cuevas, Hayley S. Thompson, Emily Dove-Meadows, and Donulae Knuckles. ‘Ubiquitous Yet Unclear: A Systematic Review of Medical Mistrust’. Behavioral Medicine (Washington, D.C.) 45, no. 2 (2019): 86–101. https://doi.org/10.1080/08964289.2019.1588220.
Bernard, Donte L., Casey D. Calhoun, Devin E. Banks, Colleen A. Halliday, Chanita Hughes-Halbert, and Carla
K. Danielson. ‘Making the “C-ACE” for a Culturally-Informed Adverse Childhood Experiences Framework to Understand the Pervasive Mental Health Impact of Racism on Black Youth’. Journal of Child & Adolescent Trauma 14, no. 2 (1 June 2021): 233–47. https://doi.org/10.1007/s40653-020-00319-9.
Bhopal, Sunil, and Maryke Nielsen. ‘Vaccine Hesitancy in Low- and Middle-Income Countries: Potential Implications for the COVID-19 Response’. Archives of Disease in Childhood, 10 September 2020. https://doi. org/10.1136/archdischild-2020-318988.
Brunson, Emily K. ‘How Parents Make Decisions about Their Children’s Vaccinations’. Vaccine 31, no. 46 (4 November 2013): 5466–70. https://doi.org/10.1016/j.vaccine.2013.08.104.
Brunson, Emily K., and Monica Schoch-Spana. ‘A Social and Behavioral Research Agenda to Facilitate COVID-19 Vaccine Uptake in the United States’. Health Security 18, no. 4 (1 August 2020): 338–44. https://doi.org/10.1089/ hs.2020.0106.
Brunson, Emily, M Schoch-Spana, M Carnes, D Hosangadi, R Long, S Ravi, M Taylor, M Trotochaud, TG Veenema, and CommuniVax Coalition. ‘Carrying Equity in COVID-19 Vaccination Forward: Guidance Informed by Communities of Color’. The Johns Hopkins University, July 2021.
Burki, Talha. ‘Vaccine Misinformation and Social Media’. The Lancet Digital Health 1, no. 6 (1 October 2019): e258–59. https://doi.org/10.1016/S2589-7500(19)30136-0.
Crenshaw, Kimberle. ‘Mapping the Margins: Intersectionality, Identity Politics, and Violence against Women of Color’. Stanford Law Review 43, no. 6 (1991): 1241–99. https://doi.org/10.2307/1229039.
Cristea, Darie, Dragoș-Georgian Ilie, Claudia Constantinescu, and Valeriu Fîrţală. ‘Vaccinating against COVID-19: The Correlation between Pro-Vaccination Attitudes and the Belief That Our Peers Want to Get Vaccinated’. Vaccines 9, no. 11 (November 2021): 1366. https://doi.org/10.3390/vaccines9111366.
Doyal, L. The Political Economy of Health. London: Pluto Press, 1979.
Dubé, Eve, Dominique Gagnon, Emily Nickels, Stanley Jeram, and Melanie Schuster. ‘Mapping Vaccine Hesitancy—Country-Specific Characteristics of a Global Phenomenon’. Vaccine 32, no. 49 (20 November 2014): 6649–54. https://doi.org/10.1016/j.vaccine.2014.09.039.
Dubé, Eve, Maryline Vivion, and Noni E. MacDonald. ‘Vaccine Hesitancy, Vaccine Refusal and the Anti-Vaccine Movement: Influence, Impact and Implications’. Expert Review of Vaccines 14, no. 1 (2 January 2015): 99–117. https://doi.org/10.1586/14760584.2015.964212.
Euser, Saskia, Floor M. Kroese, Mare Derks, and Marijn de Bruin. ‘Understanding COVID-19 Vaccination Willingness among Youth: A Survey Study in the Netherlands’. Vaccine, 5 January 2022. https://doi.org/10.1016/j. vaccine.2021.12.062.
Fazel, Mina, Stephen Puntis, Simon R. White, Alice Townsend, Karen L. Mansfield, Russell Viner, Jonathan Herring, Andrew J. Pollard, and Daniel Freeman. ‘Willingness of Children and Adolescents to Have a COVID-19 Vaccination: Results of a Large Whole Schools Survey in England’. EClinicalMedicine 40 (1 October 2021). https://doi.org/10.1016/j.eclinm.2021.101144.
Feagin, Joe, and Zinobia Bennefield. ‘Systemic Racism and U.S. Health Care’. Social Science & Medicine, Structural Stigma and Population Health, 103 (1 February 2014): 7–14. https://doi.org/10.1016/j. socscimed.2013.09.006.
Gamble, V N. ‘Under the Shadow of Tuskegee: African Americans and Health Care.’ American Journal of Public Health 87, no. 11 (November 1997): 1773–78.
Gamlin, Jennie, Jean Segata, Lina Berrio, Sahra Gibbon, and Francisco Ortega. ‘Centring a Critical Medical Anthropology of COVID-19 in Global Health Discourse’. BMJ Global Health 6, no. 6 (June 2021): e006132. https:// doi.org/10.1136/bmjgh-2021-006132.
Giles-Vernick, Tamara, Abdoulaye Traoré, and Louis Bainilago. ‘Incertitude, Hepatitis B, and Infant Vaccination in West and Central Africa’. Medical Anthropology Quarterly 30, no. 2 (2016): 203–21. https://doi.org/10.1111/ maq.12187.
Harvey, Michael. ‘The Political Economy of Health: Revisiting Its Marxian Origins to Address 21st-Century Health Inequalities’. American Journal of Public Health 111, no. 2 (1 February 2021): 293–300. https://doi.org/10.2105/ AJPH.2020.305996.
Herr, Orna. ‘Young People and Vaccine Hesitancy - What Role Does Social Media Play?’ British Science Association, 2021. https://www.britishscienceassociation.org/blog/young-people-and-vaccine-hesitancy-what- role-does-social-media-play.
Larson, Heidi J. Stuck: How Vaccine Rumors Start -- and Why They Don’t Go Away. Oxford University Press, 2020.
Larson, Heidi J., Caitlin Jarrett, Elisabeth Eckersberger, David M. D. Smith, and Pauline Paterson. ‘Understanding Vaccine Hesitancy around Vaccines and Vaccination from a Global Perspective: A Systematic Review of Published Literature, 2007–2012’. Vaccine 32, no. 19 (17 April 2014): 2150–59. https://doi.org/10.1016/j. vaccine.2014.01.081.
Leach, Melissa, and James Fairhead. Vaccine Anxieties: Global Science, Child Health and Society. Earthscan, 2007.
Middleman, Amy B., Judy Klein, and Jane Quinn. ‘Vaccine Hesitancy in the Time of COVID-19: Attitudes and Intentions of Teens and Parents Regarding the COVID-19 Vaccine’. Vaccines 10, no. 1 (January 2022): 4. https:// doi.org/10.3390/vaccines10010004.
Momplaisir, Florence, Norrisa Haynes, Hervette Nkwihoreze, Maria Nelson, Rachel M Werner, and John Jemmott. ‘Understanding Drivers of Coronavirus Disease 2019 Vaccine Hesitancy Among Blacks’. Clinical Infectious Diseases 73, no. 10 (15 November 2021): 1784–89. https://doi.org/10.1093/cid/ciab102.
OECD. ‘Enhancing Public Trust in COVID-19 Vaccination: The Role of Governments’. OECD, 2022. https:// www.oecd.org/coronavirus/policy-responses/enhancing-public-trust-in-covid-19-vaccination-the-role-of- governments-eae0ec5a/.
Packard, R. White Plague, Black Labour: Tuberculosis and the Political Economy of Health and Disease in South Africa. Oakland: University of California Press, 1989.
Siddique, Haroon, and Jessica Elgot. ‘Black, Young and Poor People in UK Most Likely to Report Covid Vaccine Hesitancy’. The Guardian, 8 March 2021, sec. Society. https://www.theguardian.com/society/2021/mar/08/ black-young-poor-people-uk-covid-vaccine-hesitancy.
Sobo, Elisa J. ‘Social Cultivation of Vaccine Refusal and Delay among Waldorf (Steiner) School Parents’. Medical Anthropology Quarterly 29, no. 3 (September 2015): 381–99. https://doi.org/10.1111/maq.12214.
Sturgis, Patrick, Lindsey Macmillan, Jake Anders, and Gill Wyness. ‘Almost Two-Thirds of Black British Young People Would Be Reluctant to Get a COVID Vaccine’. LSE COVID-19 (blog), 2021. https://blogs.lse.ac.uk/ covid19/2021/03/17/almost-two-thirds-of-black-british-young-people-would-be-reluctant-to-get-a-covid- vaccine/.
The British Academy. ‘Trust, Transparency and Data Gathering’, 2021. https://www.thebritishacademy.ac.uk/ publications/trust-transparency-data-gathering/.
The Royal Society. ‘COVID-19 Vaccine Deployment: Behaviour, Ethics, Misinformation and Policy Strategies’, October 2020.
Tourse, Robbie W.C., Johnnie Hamilton-Mason, and Nancy J. Wewiorski. Systemic Racism in the United States. Cham: Springer International Publishing, 2018. https://doi.org/10.1007/978-3-319-72233-7.
Washington, Harriet. Medical Apartheid. Penguin Random House, 2008. https://www.penguinrandomhouse. com/books/185986/medical-apartheid-by-harriet-a-washington/.
Whyte, Susan Reynolds, Sjaak van der Geest, and Anita Hardon. Social Lives of Medicines. Cambridge University Press, 2002.
Willis, Don E., Jennifer A. Andersen, Keneshia Bryant-Moore, James P. Selig, Christopher R. Long, Holly C. Felix, Geoffrey M. Curran, and Pearl A. McElfish. ‘COVID-19 Vaccine Hesitancy: Race/Ethnicity, Trust, and Fear’. Clinical and Translational Science n/a, no. n/a (2021). https://doi.org/10.1111/cts.13077.
Citations
- Marcia J Ash et al., ‘Predictors of Medical Mistrust among Urban Youth of Color during the COVID-19 Pandemic’, Translational Behavioral Medicine, 3 June 2021, ibab061, https://doi.org/10.1093/tbm/ibab061.
- Saskia Euser et al., ‘Understanding COVID-19 Vaccination Willingness among Youth: A Survey Study in the Netherlands’, Vaccine, 5 January 2022, https://doi.org/10.1016/j.vaccine.2021.12.062.
- Amy B. Middleman, Judy Klein, and Jane Quinn, ‘Vaccine Hesitancy in the Time of COVID-19: Attitudes and Intentions of Teens and Parents Regarding the COVID-19 Vaccine’, Vaccines 10, no. 1 (January 2022): 4, https://doi.org/10.3390/vaccines10010004.
- Talha Burki, ‘Vaccine Misinformation and Social Media’, The Lancet Digital Health 1, no. 6 (1 October 2019): e258–59, https://doi.org/10.1016/ S2589-7500(19)30136-0.
- Sunil Bhopal and Maryke Nielsen, ‘Vaccine Hesitancy in Low- and Middle-Income Countries: Potential Implications for the COVID-19 Response’, Archives of Disease in Childhood, 10 September 2020, https://doi.org/10.1136/archdischild-2020-318988; Eve Dubé, Maryline Vivion, and Noni E. MacDonald, ‘Vaccine Hesitancy, Vaccine Refusal and the Anti-Vaccine Movement: Influence, Impact and Implications’, Expert Review of Vaccines 14, no. 1 (2 January 2015): 99–117, https://doi.org/10.1586/14760584.2015.964212; Eve Dubé et al., ‘Mapping Vaccine Hesitancy—Country-Specific Characteristics of a Global Phenomenon’, Vaccine 32, no. 49 (20 November 2014): 6649–54, https:// doi.org/10.1016/j.vaccine.2014.09.039.
- Emily Brunson et al., ‘Carrying Equity in COVID-19 Vaccination Forward: Guidance Informed by Communities of Color’ (The Johns Hopkins University, July 2021); Heidi J. Larson, Stuck: How Vaccine Rumors Start -- and Why They Don’t Go Away (Oxford University Press, 2020); Melissa Leach and James Fairhead, Vaccine Anxieties: Global Science, Child Health and Society (Earthscan, 2007).
- Brunson et al., ‘Carrying Equity in COVID-19 Vaccination Forward: Guidance Informed by Communities of Color’.
- Heidi J. Larson et al., ‘Understanding Vaccine Hesitancy around Vaccines and Vaccination from a Global Perspective: A Systematic Review of Published Literature, 2007–2012’, Vaccine 32, no. 19 (17 April 2014): 2150–59, https://doi.org/10.1016/j.vaccine.2014.01.081.
- Donte L. Bernard et al., ‘Making the “C-ACE” for a Culturally-Informed Adverse Childhood Experiences Framework to Understand the Pervasive Mental Health Impact of Racism on Black Youth’, Journal of Child & Adolescent Trauma 14, no. 2 (1 June 2021): 233–47, https://doi. org/10.1007/s40653-020-00319-9.
- Mina Fazel et al., ‘Willingness of Children and Adolescents to Have a COVID-19 Vaccination: Results of a Large Whole Schools Survey in England’, EClinicalMedicine 40 (1 October 2021), https://doi.org/10.1016/j.eclinm.2021.101144; Haroon Siddique and Jessica Elgot, ‘Black, Young and Poor People in UK Most Likely to Report Covid Vaccine Hesitancy’, The Guardian, 8 March 2021, sec. Society, https://www. theguardian.com/society/2021/mar/08/black-young-poor-people-uk-covid-vaccine-hesitancy.
- Patrick Sturgis et al., ‘Almost Two-Thirds of Black British Young People Would Be Reluctant to Get a COVID Vaccine’, LSE COVID-19 (blog), 2021, https://blogs.lse.ac.uk/covid19/2021/03/17/almost-two-thirds-of-black-british-young-people-would-be-reluctant-to-get-a-covid- vaccine/.
- Joe Feagin and Zinobia Bennefield, ‘Systemic Racism and U.S. Health Care’, Social Science & Medicine, Structural Stigma and Population Health, 103 (1 February 2014): 7–14, https://doi.org/10.1016/j.socscimed.2013.09.006; Harriet Washington, Medical Apartheid (Penguin Random House, 2008), https://www.penguinrandomhouse.com/books/185986/medical-apartheid-by-harriet-a-washington/.
- Robbie W.C. Tourse, Johnnie Hamilton-Mason, and Nancy J. Wewiorski, Systemic Racism in the United States (Cham: Springer International Publishing, 2018), https://doi.org/10.1007/978-3-319-72233-7.
- Kimberle Crenshaw, ‘Mapping the Margins: Intersectionality, Identity Politics, and Violence against Women of Color’, Stanford Law Review 43, no. 6 (1991): 1241–99, https://doi.org/10.2307/1229039.
- Brunson et al., ‘Carrying Equity in COVID-19 Vaccination Forward: Guidance Informed by Communities of Color’.
- The Royal Society, ‘COVID-19 Vaccine Deployment: Behaviour, Ethics, Misinformation and Policy Strategies’, October 2020; The British Academy, ‘Trust, Transparency and Data Gathering’, 2021, https://www.thebritishacademy.ac.uk/publications/trust-transparency-data- gathering/.
- Larson et al., ‘Understanding Vaccine Hesitancy around Vaccines and Vaccination from a Global Perspective’.
- Don E. Willis et al., ‘COVID-19 Vaccine Hesitancy: Race/Ethnicity, Trust, and Fear’, Clinical and Translational Science n/a, no. n/a (2021), https://doi.org/10.1111/cts.13077.
- Florence Momplaisir et al., ‘Understanding Drivers of Coronavirus Disease 2019 Vaccine Hesitancy Among Blacks’, Clinical Infectious Diseases 73, no. 10 (15 November 2021): 1784–89, https://doi.org/10.1093/cid/ciab102.
- Sirry Alang, Donna D. McAlpine, and Rachel Hardeman, ‘Police Brutality and Mistrust in Medical Institutions’, Journal of Racial and Ethnic Health Disparities 7, no. 4 (1 August 2020): 760–68, https://doi.org/10.1007/s40615-020-00706-w.
- Ash et al., ‘Predictors of Medical Mistrust among Urban Youth of Color during the COVID-19 Pandemic’.
- Brunson et al., ‘Carrying Equity in COVID-19 Vaccination Forward: Guidance Informed by Communities of Color’; Dubé, Vivion, and MacDonald, ‘Vaccine Hesitancy, Vaccine Refusal and the Anti-Vaccine Movement’; Leach and Fairhead, Vaccine Anxieties; Elisa J. Sobo, ‘Social Cultivation of Vaccine Refusal and Delay among Waldorf (Steiner) School Parents’, Medical Anthropology Quarterly 29, no. 3 (September 2015): 381–99, https://doi.org/10.1111/maq.12214.
- Jennie Gamlin et al., ‘Centring a Critical Medical Anthropology of COVID-19 in Global Health Discourse’, BMJ Global Health 6, no. 6 (June 2021): e006132, https://doi.org/10.1136/bmjgh-2021-006132.
- L. Doyal, The Political Economy of Health (London: Pluto Press, 1979); Michael Harvey, ‘The Political Economy of Health: Revisiting Its Marxian Origins to Address 21st-Century Health Inequalities’, American Journal of Public Health 111, no. 2 (1 February 2021): 293–300, https://doi.org/10.2105/AJPH.2020.305996; R. Packard, White Plague, Black Labour: Tuberculosis and the Political Economy of Health and Disease in South Africa (Oakland: University of California Press, 1989).
- Gamlin et al., ‘Centring a Critical Medical Anthropology of COVID-19 in Global Health Discourse’.
- Gamlin et al., ‘Centring a Critical Medical Anthropology of COVID-19 in Global Health Discourse’.
- Lesley Bartlett and Frances Vavrus, Rethinking Case Study Research: A Comparative Approach (New York: Routledge, 2016), https://doi. org/10.4324/9781315674889.
- Orna Herr, ‘Young People and Vaccine Hesitancy - What Role Does Social Media Play?’, British Science Association, 2021, https://www. britishscienceassociation.org/blog/young-people-and-vaccine-hesitancy-what-role-does-social-media-play.
- Emily K. Brunson, ‘How Parents Make Decisions about Their Children’s Vaccinations’, Vaccine 31, no. 46 (4 November 2013): 5466–70, https://doi.org/10.1016/j.vaccine.2013.08.104; Sobo, ‘Social Cultivation of Vaccine Refusal and Delay among Waldorf (Steiner) School Parents’.
- Darie Cristea et al., ‘Vaccinating against COVID-19: The Correlation between Pro-Vaccination Attitudes and the Belief That Our Peers Want to Get Vaccinated’, Vaccines 9, no. 11 (November 2021): 1366, https://doi.org/10.3390/vaccines9111366; Euser et al., ‘Understanding COVID-19 Vaccination Willingness among Youth’.
- Tamara Giles-Vernick, Abdoulaye Traoré, and Louis Bainilago. ‘Incertitude, Hepatitis B, and Infant Vaccination in West and Central Africa’. Medical Anthropology Quarterly 30, no. 2 (2016): 203–21. https://doi.org/10.1111/maq.12187.
- Susan Reynolds Whyte, Sjaak van der Geest, and Anita Hardon, Social Lives of Medicines (Cambridge University Press, 2002).
- Emily K. Brunson and Monica Schoch-Spana, ‘A Social and Behavioral Research Agenda to Facilitate COVID-19 Vaccine Uptake in the United States’, Health Security 18, no. 4 (1 August 2020): 338–44, https://doi.org/10.1089/hs.2020.0106.
- Ramona Benkert et al., ‘Ubiquitous Yet Unclear: A Systematic Review of Medical Mistrust’, Behavioral Medicine (Washington, D.C.) 45, no. 2 (2019): 86–101, https://doi.org/10.1080/08964289.2019.1588220; V N Gamble, ‘Under the Shadow of Tuskegee: African Americans and Health Care.’, American Journal of Public Health 87, no. 11 (November 1997): 1773–78.
- Alang, McAlpine, and Hardeman, ‘Police Brutality and Mistrust in Medical Institutions’.
- Brunson and Schoch-Spana, ‘A Social and Behavioral Research Agenda to Facilitate COVID-19 Vaccine Uptake in the United States’.
- Alang, McAlpine, and Hardeman, ‘Police Brutality and Mistrust in Medical Institutions’.
- OECD, ‘Enhancing Public Trust in COVID-19 Vaccination: The Role of Governments’, OECD, 2022, https://www.oecd.org/coronavirus/ policy-responses/enhancing-public-trust-in-covid-19-vaccination-the-role-of-governments-eae0ec5a/.
- OECD, ‘Enhancing Public Trust in COVID-19 Vaccination’.
Summary
- Published
© The authors. This is an open access publication licensed under a Creative Commons Attribution-NonCommercial- NoDerivs 4.0 Unported License
To cite this report: British Academy (2022), The COVID-19 YPAR Project: Youth Participatory Action Research (YPAR) to explore the context of ethnic minority youth responses to COVID-19 vaccines in the United States and United Kingdom, The British Academy, London
- DOI doi.org/10.5871/c19-recovery/M-S-S-T-H-E-B-JM-S-T-B-A-J-S (Opens in a new window)