Securing the Goalposts on Vaccine Hesitancy
COVID-19 Recovery: Building Future Pandemic Preparedness and Understanding Citizen Engagement in the
USA and UK
By Andy Brownback, Guillermo Cruces, Seung-Keun Martinez, Monika Pompeo and Silvia Sonderegger
Download PDF report
- Published by
- British Academy
- Year
- 2022
- Pages
- 24
About the authors
Professor Silvia Sonderegger is Professor of Economics at the University of Nottingham. Professor Guillermo Cruces is Professor of Economics at the University of Nottingham. Dr Seung-Keun Martinez is an Assistant Professor at the University of Nottingham. Dr Andy Brownback is an Associate Professor at the University of Arkansas. Monika Pompeo is a PhD Student at the University of Nottingham.
About the COVID-19 Recovery: Building Future Pandemic Preparedness and Understanding Citizen Engagement in the USA and UK
The programme is the result of a partnership between the British Academy, the Social Sciences Research Council (SSRC) and the Science & Innovation Network in the USA (SIN USA) to award funding to ten transatlantic studies focusing on UK-US COVID-19 vaccine engagement. It follows a pilot study exploring levels of vaccine engagement in four locations across the US and UK, while the larger programme was expanded to study multiple locations. The programme was funded by the UK’s Department for Business, Energy and Industrial Strategy.
Abstract
In this project, we quantitatively assessed how vaccine hesitancy is influenced by (i) a lack of information on COVID-19 and its vaccines, and (ii) politically-motivated reasoning or exposure to misinformation. We tested scalable interventions to address both of these potential causes of vaccine hesitancy using a large-scale (n=8000) randomized control trial run on unvaccinated populations in both UK and US. The key outcomes of this trial were attitudes towards vaccination and willingness to seek further information. Our first intervention addressed information gaps through a series of comprehensive but accessible animated videos about COVID-19 and its vaccines. For both the UK and US, we found that these videos cause positive changes in attitudes towards vaccines and intentions to be vaccinated. Furthermore, we observed that a large share of participants (approximately 60%) engaged in further information seeking by watching additional (non-compulsory) videos on COVID-19 vaccination. Our second intervention addressed politically-motivated reasoning by adapting the communication tools of “Paradoxical Reasoning” which were developed to unfreeze entrenched beliefs in the context of the most intractable conflicts (e.g., the Israeli-Palestinian border conflict). In our US sample, we found that this communication method caused positive changes in vaccine intentions. In contrast, in the UK, it had no effect (and even a negative effect in some dimensions). In addition to effective interventions, we developed a metric of motivated reasoning that we hope will allow healthcare providers to identify which individuals are more likely to be resistant to standard information provision about the vaccine. We validate this metric by showing its predictive validity for individual attitudes towards the vaccine.
Executive summary
Our study used a randomized controlled trial, viewed by some as the gold-standard approach to social-science research, to provide robust, scientific evidence on the effectiveness of two interventions designed to improve attitudes towards COVID-19 vaccines among unvaccinated individuals. We additionally developed a novel metric for predicting a person’s attitudes towards the vaccine.
Treatment 1: video interventions
We developed four short videos that present key information about COVID-19 vaccines, their development, testing, and side effects. These were short (approx. 2 minutes) comprehensive videos with a careful yet easy-to-grasp treatment of technical details, delivered in a format (animation) that made them accessible to the general public.
Our intervention required that subjects view one video and presented them with the opportunity to view additional videos. This limited exposure had a strong impact. Relative to an untreated control group, in both UK and US we observe that exposure to the video significantly improved vaccine perceptions. For instance, perceptions of vaccine effectiveness increased by approximately 13% in both countries. Furthermore, despite the technical content and the general anti-vaccination stance of our sample, nearly 60% of our subjects chose to watch additional videos about the COVID-19 vaccines on their own time. On average, subjects watched more than twice as many videos as were required.
Key finding: In both the UK and US, exposing subjects to detailed but approachable videos had a positive influence on attitudes about vaccination. The interventions were engaging enough that unvaccinated viewers willingly sought out additional (non- compulsory) videos.
Treatment 2: paradoxical reasoning
Alongside our video intervention, we developed “paradoxical reasoning” interventions that engaged our subjects in a reductio-ad-absurdum dialogue about anti-vaccination positions. These interventions required our subjects to engage with the most extreme anti-vaccination views in a way designed to soften positions around this politically charged topic.
The effect of this intervention differed between countries: In the US, the intervention significantly improved vaccination intentions. The effect on vaccine intentions of paradoxical reasoning was actually larger than the effect of the video intervention (7.4% versus 4.7%). In the UK, on the other hand, we found that exposure to paradoxical reasoning did not improve perceptions and actually worsened them in some dimensions. We hypothesize that this difference is due to the different nature of vaccine hesitancy between the two countries. In the US, the debate surrounding vaccination has been heavily politicized, with partisan media accusing the opposing faction of spreading misinformation and fake news, something that has not occurred in the UK.
Key finding: Paradoxical interventions worked well in the US but not in the UK.
Diagnostic tool: motivated reasoning metric
We developed a metric we could use to predict how a subject’s tendency to engage in motivated reasoning (ex-post rationalization to their own positions) might affect their views on vaccination. This metric was based on observed inconsistencies in the subjects’ concerns about vaccination. Motivated reasoners are especially interesting because they are by nature quite resistant to information. In both countries, we found that our metric predicted more negative vaccine perceptions. Furthermore, we found that, in the US, Republicans exhibited a higher incidence of motivated reasoning compared to Democrats. For the UK we did not identify any meaningful pattern of motivated reasoning, possibly reflecting the fact that, relative to the US, the UK does not feature such strong political divides, especially when it comes to the rhetoric and public discourse surrounding vaccination.
Key finding: We developed an index of motivated reasoning which is effective in predicting more negative attitudes towards the vaccine.
Policy implications
Our analysis delivers a number of important policy implications.
- A little exposure can go far - Exposing vaccine resistant individuals to a short, simple but scientifically rigorous videos resulted in a large share of individuals (60%) seeking out further videos.
- Paradoxical interventions don’t work for everyone - Although exposure to paradoxical interventions significantly improved vaccination intentions in the US, this was not the case for the UK. The likely cause for this difference lies in the different makeup of vaccine hesitant populations in the two countries.
- Trying too hard may backfire - Mixing videos and paradoxical reasoning had a backfire effect on vaccine attitudes. This suggests that there may be decreasing returns from superimposing different types of interventions, perhaps arising from induced fatigue in our subjects.
- Two paradoxes are better than one - In the US, exposing subjects to two paradoxical interventions instead of one reinforced the positive effect on vaccine intentions.
- Mode of information delivery matters - Our interventions worked equally well on motivated reasoners as on the rest of our subjects. This suggests that the manner in which we packaged our interventions – in the form of animation videos explaining the underlying technology behind vaccines, or of paradoxical interventions leading to somewhat absurd anti-vaccine conclusions – made them less conducive to adverse ad-hoc reactions by motivated reasoners
Introduction
There is a clear scientific consensus that COVID 19 vaccines are safe and effective in fighting this pernicious disease.(1) Although this information is readily available, as of this writing only approximately 65% of eligible individuals in the United States have been fully vaccinated, with fewer than half of eligible individuals being vaccinated in several states.(2) This is despite the fully FDA approved Pfizer/BioNTech vaccine being ubiquitously available, approximately 1-in-500 Americans having died from the virus, and proliferating vaccine mandates. While the UK has had greater success in its vaccination campaign, about half of those who remain unvaccinated in both countries state they never intend to get the vaccine.(3) Indeed, as has been discussed and documented, most developed countries have reached a plateau of vaccine compliance.(4)
In the United States, the disparity in vaccination rates appears greatest along political, social, religious, and geographical divides. For instance, 69% of the general public, 88% of Democrats, 55% of Republicans, 52% of rural residents, 79% of urban residents, 76% of black Americans, 71% of Latino Americans, 66% of white Americans, and 59% of white evangelicals self-report being vaccinated.(5) Recognizing that there is a strong correlation between race, geography, and political affiliation, the evidence can be rationalized by the following competing hypotheses:
- Vaccine-resistant individuals and vaccine-resistant communities have not yet updated their beliefs about COVID-19 and the threat it poses.
- Beliefs about the threat of COVID-19 and the importance of vaccination are entrenched along political and social lines.
These competing hypotheses require drastically different solutions. The first requires that trusted local sources disseminate up-to-date information on the threat of COVID-19 that is specifically tailored towards individual communities. The second may require more unorthodox interventions designed to unfreeze politically motivated and entrenched beliefs.
The purpose of our project was to understand the underlying motivations behind those who remain unvaccinated and develop a communication and media toolkit to aid frontline healthcare workers engage their most adamantly vaccine resistant patients. We believe our results could lead to large scale programs and interventions and open the door to further research on this vital topic.
While the UK has experienced considerably less COVID-19 vaccine hesitancy, evidence suggests there may be similar motivations between those who remain unvaccinated in both countries. In particular, Portat et al. show that government policies that threaten autonomy, e.g. vaccine passports, may increase hesitancy among certain individuals.(6) Similar sentiment can easily be observed in American conservative media on the White House’s recent vaccine mandates.(7) The first goal of our project was to assess whether the vaccine hesitant can be reached with standard messaging. If many of those who remain unvaccinated simply feel confused by the evolving messaging of media outlets or struggle to determine which information is medically accurate, then listening to the concerns of hesitant individuals and building an easily accessible tool may increase vaccine confidence and uptake. This tool presents the decision to vaccinate along three questions.
- How much of a threat is COVID-19 to your health?
- How effective is the vaccine?
- Is the vaccine safe?
In our more standard interventions, we provided easily understandable information that directly addresses these questions with the intent of allowing individuals to reach informed conclusions on straightforward criteria. Rather than simply providing a list of unverifiable statements or hard-to-grasp data on vaccine safety, we used video animation to explain the underlying vaccination technology in a scientifically sound yet easily comprehensible way.
At the same time, it is also possible that many of those who have refused the vaccine have engaged in politically motivated reasoning to support their decision. In preliminary conversations with medical doctors, we found that it is a common frustration that their patients refuse to engage with good faith conversations on vaccination, will question the reliability of the doctor’s knowledge, and will refer to fringe and unvalidated theories to rationalize their choices. After all, as more and more evidence in favour of vaccination emerges, a sure-fire strategy to justify remaining unvaccinated is to move the goal posts on what evidence is required to demonstrate that the COVID-19 vaccine is safe and effective and to reject any pro- vaccination information as “fake news”.
In light of this challenge, we hoped to create an effective toolkit for engaging vaccine hesitant individuals and communities. In addition to a survey of concerns and an informational intervention in the form of custom-made information videos, we employed a complementary technique from the political psychology literature.
Previous studies have found that political misperceptions can be corrected by detailing an alternative causal chain of events,(8) and exposing individuals to exaggerated or even absurd ideas that align with their beliefs can be an effective intervention, especially among individuals who are adamant in their views.9 In our methodology section we refer to this approach as “paradoxical reasoning”. It is with this toolkit that we hoped to aid doctors, nurses, and community health workers engage highly vaccine hesitant individuals.
Our sample
Our study consisted of a large-scale online experiment with approximately 8,000 unvaccinated subjects (7000 from the US and 1000 from the UK). The data were collected in January/February 2022. Our focus on unvaccinated individuals allows us to assess the effect of our interventions on those individuals who exhibit the strongest form of vaccine resistance. Subjects were randomly recruited from two online survey companies, Lucid and Prolific.(10) A full breakdown of demographic characteristics of our UK and US samples is available in the longer version of the report.
Interventions
3.1 Video intervention
We designed four custom videos of approximately 2 minutes each to address information gaps in the communications about COVID-19 vaccines. The videos were devised to be both scientifically sound and at the same time accessible for the average individual. Rather than making unverifiable statements on vaccine safety or exposing our subjects to hard-to-interpret data, we focused on explaining the underlying technology at work in vaccines in an accurate, yet simple and accessible way. We commissioned an animation professional to design animated videos to complement the spoken script. This proved particularly useful for explaining relatively complex scientific ideas. The videos are described in some detail below:
Vaccine Technology video: described the mRNA technology behind COVID-19 vaccines.
Vaccine Development video: explained how the COVID-19 vaccines were researched and developed. It also compares the rapid development of COVID-19 vaccines to the more time-consuming development of older, more traditional vaccines, and discusses how potential variant-specific boosters would be made.
Vaccine Testing video: explained how COVID-19 vaccines were tested for FDA review and how this process was accelerated in comparison to how new drugs and vaccines are normally tested.
Side Effects video: explained why side effects arise and discusses the prospects of long-term side effects and serious adverse events.
Subjects were randomly assigned to one of the following treatments; Video Required, Video Control and Video Optional.
- Video Required condition: in our main treatment subjects watched the Technology video. After watching this video, they were given the choice to watch as many of the three remaining informational videos as they liked, or they could choose not to watch any additional videos at all.
- Video Control treatment: to evaluate the effect of video exposure on vaccine attitudes, we also ran a placebo treatment of the same length and made in the same style as our vaccine videos. The placebo video was unrelated to Covid or vaccination and instead covered how to solve a simple logic puzzle.
- Video Optional treatment: finally, we also ran a treatment where subjects watched the same placebo video as in the Video Control condition and, in addition, were also offered the choice to select any of our four vaccine information videos. They were able to watch as many of the four information videos as they liked, or they could choose not to watch any at all. The Video Optional treatment was not our main focus of interest but was run to verify whether, in practice, subjects who had not been required to watch any of our information videos would nonetheless engage with them.
Due to the smaller number of observations, in the UK sample, the Video Optional condition was not run. Subjects were randomly assigned either to Video Required or to Video Control. In the US sample, subjects could be randomly assigned to any of the three treatments described above, although the majority were assigned to either Video Control or Video Required. That’s because the Video Required treatment allowed us to test the effect of our video intervention on those among our subjects who would normally not have chosen to watch an informative video on Covid vaccination of their own accord. At the same time, we were aware that exposing the subjects to too much information could cause a backlash effect due to “intervention overloading”. For this reason, in the Video Required treatment we only asked our subjects to watch one video, letting them choose of their own volition whether they wished to view any more. As we explain below, a rather large share of subjects (60%) actually chose to do so.
3.2 Paradoxical reasoning interventions
We designed two paradoxical reasoning interventions in the form of written text prompting subjects to engage with an argument that supports increasingly extreme viewpoints through an approach similar to a reductio-ad-absurdum. This type of intervention has been shown to soften views towards intractable conflicts such as the Israeli-Palestinian conflict. Our paradoxes were:
Natural Immunity Paradox: asked respondents to consider whether or not achieving natural immunity through deliberately catching COVID-19 is a good idea.
Long-Run Testing: asked respondents to consider whether 18 months of data on a vaccine is enough or if we should not approve any vaccine until it has undergone long enough testing to last the majority of a recipient’s lifetime.
The experiment included the following four paradox treatments:
- Paradox Control Condition (PC ) In this condition, the subjects interacted with a placebo protocol that asks the same number of questions in the same progressive manner as the paradoxical reasoning interventions but does not relate to COVID-19 vaccines.
- Natural Immunity Paradox (PNI ) In this condition, subjects were presented with the Natural Immunity Paradox.
- Long-Run Paradox (PLR ) In this condition, subjects were presented with the Long-Run Paradox.
- Both Paradoxes (PB ) In this condition, subjects were presented with both the Natural Immunity Paradox and the Long-Run Paradox.
Due to the smaller number of observations, in the UK sample, we eliminated the single paradox conditions PNI and PLR . Subjects were randomly assigned either to the PC or the PB conditions. In the US sample, subjects could be randomly assigned to any of the four conditions described above (although the majority were assigned to either PC or PB ).
3.3 Mixed interventions
In the UK sample subjects were either randomly exposed to the paradox intervention (in the form of PB ) or the video intervention (in the form of V2 ), but not both. Instead, in the US sample, subjects could be randomly exposed to both types of interventions.
Data collection
We now describe our online survey in detail, describing how the data were subsequently used in our analysis.
4.1 Covid perceptions
We collected each subject’s perceptions about COVID-19, including their beliefs about its severity, the benefits or risks of vaccination, and the trustworthiness of institutions, as follows. These questions were used to construct three primary indices for evaluating perceptions surrounding vaccination.(12) These were (1) Perception[1]: measuring vaccination intentions and concerns; (2) Perception[2]: measuring perception of vaccination efficacy; (3) Perception[3]: measuring concerns over vaccination side effects. Perception[1] was our most important outcome, capturing vaccination intentions and concerns which are of primary policy relevance. Second, beliefs about vaccine efficacy Perception [2] were also measured – the underlying idea being that these beliefs play an important role in vaccine take-up. Finally, we measured the subjects’ concerns about possible side effects of vaccination Perception [3]. These are relevant in that they may limit the effectiveness of vaccination efforts.
4.2 Motivated reasoning
We used the responses to our questionnaire to build an index of motivated reasoning, defined as the (conscious or unconscious) tendency to justify vaccine-resistance by forming ad-hoc beliefs that rationalize it. Motivated reasoning has been observed for instance in the political sphere(13) as well as in financial markets and other environments.(14) Our focus was on constrained motivated reasoners, namely individuals who are not totally immune to information but may nonetheless be subject to biases that may prevent them from fully taking into account information which contrasts with their current position. For instance, a subject receiving information on how rare vaccine-induced myocarditis is might engage in motivated reasoning by overstating their concern about vaccination-induced risk of blood clots, in order to justify their attitudes towards vaccination. The underlying idea is that being exposed to factual information indicating that vaccine are safe in a given dimension increases the cost of motivated reasoning in that dimension. In order to justify their vaccine resistance, constrained motivated reasoners then react by inflating their concerns over vaccine safety in another dimension. The methodology we used to construct our index of motivated reasoning is explained in detail in the long version of the report. In our analysis, we were interested in assessing the effect that our interventions can operate on motivated reasoners, potentially breaking down their barriers and positively affecting their attitudes towards vaccination.
4.3 Social group perceptions
We constructed an index of social perceptions based on a set of questions measuring the strength of vaccine resistance among a subject’s social group
4.4 Information-seeking behaviour
Two of our video treatments (Video Required and Video Optional) allowed subjects to elect to watch additional videos after their first mandatory video. We measured their information-seeking behaviour as the number of subsequent videos watched after the first.
How did vaccine perceptions vary by demographic characteristics?
We start our analysis by reporting on the relationship between our indexes of Covid perceptions and demographic characteristics. We uncovered a number of interesting patterns common to our subjects across both UK and US:
- Controlling for other demographic characteristics (such as age, ethnicity, education, gender etc), subjects who side with the opposition party (in US: Republican, in UK: Labour) hold more negative attitudes towards the vaccine – in terms of our three perception indices and trust in healthcare authorities – than subjects belonging to the party currently in power. This is presumably due to individuals viewing vaccines more negatively when they have a negative opinion of the government response to the Covid crisis (something that is more likely to happen among members of the opposition party). The cross-party difference in perceptions that we observe in the US is about twice the difference observed in the UK, reflecting a wider political divide on vaccine issues.
We also find that, in the US:
- Subjects belonging to racial minorities (both Black and Non-Black) score higher for Perception1, our primary measure, capturing vaccination intentions and concerns. This suggests that, in the US, unvaccinated racial minorities tend to exhibit a lower degree of resistance to the vaccine than unvaccinated Caucasian individuals (in the UK we find no significant difference).
- Subjects from rural areas tend to be more negative towards vaccination. This is especially apparent for subjects coming from the rural West, whose attitudes (in terms of all our vaccine perception indices and their trust in healthcare authorities) are significantly more negative than those of subjects from any other area (rural or urban).(15) In the UK, the geographic patterns we observe are not as strongly defined as in the US, although subjects from the South of England appear to be somewhat more positively inclined towards the vaccine than the rest of the country, in particular the Midlands and the North of England (and, to a lesser extent, London).
5.1 Social perception index
We now turn to our social perception index, measuring the strength of anti-vaccine prejudice in a subject’s social group. In both countries, we find that more educated subjects tend to interact with social groups that are less anti-vaccine.(16) In the US, the same is true of Non-Black minorities, subjects located in the Northeast (compared to all other areas), subjects living in urban areas (compared to rural) and Democrats/ Independents (compared to Republicans). In contrast, in the UK, we find that subjects belonging to racial minorities (Black and Non-Black) tend to move in social circles that are more vaccine-negative compared to their Caucasian counterparts. Moreover, again in contrast with the US findings, subjects living in rural UK areas interact in social groups that are generally are less anti-vaccine compared to subjects living in urban areas.
5.2 Motivated reasoning
The main pattern we identify in our US data in terms of tendency to engage in motivated reasoning cuts across political lines: Republicans are significantly more likely to engage in motivated reasoning compared to Democrats. We also identify a tendency of subjects belonging to a Non-Black racial minority to be less likely to engage in motivated reasoning compared to Caucasians, although the effect is weaker than that of political affiliation. For the UK we do not identify any meaningful pattern of motivated reasoning, possibly reflecting the fact that, relative to the US, the UK does not feature such strong political divide, especially when it comes to the rhetoric and public discourse surrounding vaccination.
Effects of interventions
6.1 Video intervention
In the US, our Video Required intervention generated statistically significant improvements in our subjects’ scores in all our three vaccine perception indices. The effect is largest for Perception2 (where we observed an improvement of 12.6% compared to the control group) followed by Perception3 (9.4% improvement) and then by Perception1 (4.7% improvement) where the effect is positive but least pronounced. Perceptions also improved in the Video Optional treatment, probably due to the fact that a good share chose to watch some of our videos also in that case.(17) In the UK, the effect of our video intervention was also positive but is statistically significant only for Perception2 (where we observed a 13% improvement compared to the control group) possibly due to a smaller number of observations.
6.2 Paradoxical reasoning intervention
Exposure to paradoxical reasoning generated a statistically significant increment in our US subjects’ Perception1 index, which reflects our most important outcome variable, namely vaccination intentions. For this variable, the effect of paradoxical intervention was larger and stronger than the effect of the video intervention (7.4% improvement compared to the control group), suggesting that our paradoxical approach achieved a better result in moving the vaccine intentions of vaccine- hesitant individuals compared the more standard video intervention.(18) We used the first wave of US data (approx. 4000 observations) to investigate whether exposure to more than one paradox could create some backlash effect. We found no evidence that being presented with both paradoxes made things worse, in fact, we observed that in some cases it produced a stronger positive effect compared to one paradox alone. For that reason, in the second US data-collection wave and in the UK sample, we eliminated the single-paradox conditions (PNI and PLR), focusing instead only on exposing subjects either to both paradoxes (PB) or the control condition (PC).
In contrast to what was observed in the US, in the UK we found no positive evidence that the paradoxical reasoning intervention had a positive effect on our subjects’ vaccine perceptions. If anything, this intervention appears to lower our subjects’ Perception2 index, whilst leaving the other indices unchanged. We hypothesize that this difference is due to the different nature of vaccine hesitancy between the two countries. In the US, the debate surrounding vaccination has been heavily politicized, with partisan media accusing the opposing faction of spreading misinformation and fake news, something that has not occurred in the UK. Accordingly, in the US, vaccine-hesitant individuals may be much more responsive to non-traditional types of intervention – such as paradoxical reasoning – which do not give the impression of being geared towards changing the mind of the responder.
6.3 Interaction between video and paradoxical reasoning
Our evidence indicates that interacting the video and paradox treatments does not improve and in some cases actually worsens our vaccine perceptions indices, compared to the case in which we introduce only one intervention. This suggests that there may be decreasing returns from superimposing different types of interventions, perhaps arising from induced fatigue in our subjects. In other words, trying too hard may backfire when it comes to changing the attitudes of vaccine resistant individuals.
6.4 Interaction with motivated reasoning
In the US, a higher index of motivated reasoning significantly lowered our subjects’ perception indices as well as their trust in healthcare institutions. In other words, motivated reasoning shifted vaccine perceptions downwards (by around 5-10% depending on the indices). In the UK, the effect went in the same direction but was weaker. These observations validate our metric, by showing its predictive validity for individual attitudes towards the vaccine.
Remarkably, in both countries, we failed to identify any significant interaction between motivated reasoning and our treatments. This implies that the effect of our interventions on vaccine perceptions was the same independently of whether subjects engaged or not in motivated reasoning. Although motivated reasoners were found to selectively adjust their beliefs to counteract the effect of information in the form of pro-vaccine data, when confronted with our video or paradoxical interventions their reaction was unbiased, resulting in an improvement in vaccine perceptions comparable to that of individuals who are not motivated reasoners. This suggests that the manner in which we packaged our interventions – in the form of animation videos explaining the underlying technology behind vaccines, or of paradoxical interventions leading to somewhat absurd anti-vaccine conclusions – made them less conducive to adverse ad-hoc reactions by motivated reasoners.
6.5 Information seeking
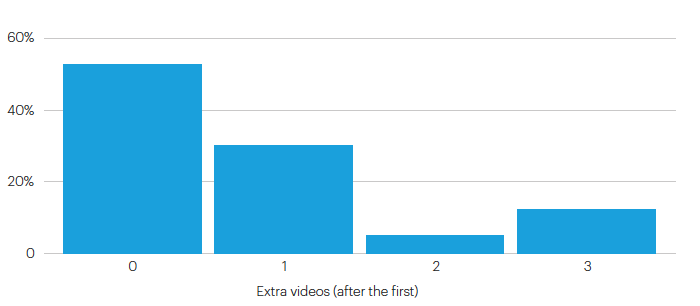
In both the UK and US, around 60% of subjects in the Video Required treatment chose to watch additional (non-compulsory) videos on vaccine-related themes after they had watched the first one. In addition, when the first video was optional (Video Optional treatment), approximately 50% of subjects chose to watch at least one video, and around 30% chose to watch at least two. Around one-third (resp., one fifth) of subjects watched all four videos in the Video Required (resp., Video Optional) treatment. These are remarkable figures, especially given the fact we are working with unvaccinated individuals, who represent the most vaccine-resistant portion of the population.
Figure 1: Information seeking behaviour in the US sample
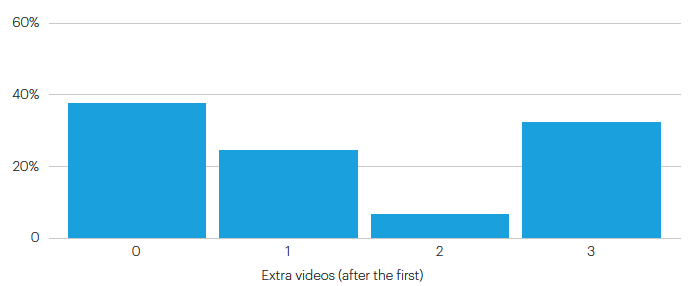
Figure 2: Information seeking behaviour in UK sample
6.6 Evidence from follow-up survey
We ran a follow-up survey to measure additional effects of our interventions. To this purpose, approximately one week after the initial survey, we recontacted our US subjects to ask about any developments concerning vaccination. When considering the positions expressed by those who replied to our recontacting invitation, we found that subjects who had been exposed to our interventions continued to exhibit more positive attitudes towards vaccination compared to the placebo group. The increment in our primary measure, vaccination intentions, was similar to that of our main study, and was larger for paradoxical intervention. However, presumably due to the smaller sample size, these effects were not as precisely estimated as they were in the main study.(19)
Concluding remarks
In this study, we designed and tested two types of interventions on unvaccinated subjects both in the US and the UK. Our aim was to investigate whether the perceptions of vaccine resistant populations could be improved by means of a targeted and somewhat unorthodox approach. We considered two types of interventions.
First, a video intervention where subjects are introduced to the underlying technology behind vaccines in an approachable and down-to-earth manner. The videos exploited animated images to complement the voice-over explanations and to achieve the transmission of relatively complex concepts in the easiest and most direct way.
Second, we considered a less standard type of intervention in the form of “paradoxical reasoning”, namely a reductio-ad-absurdum reasoning process where subjects are exposed to increasingly extreme implications of their anti-vaccine positions.
While the video intervention was successful in both countries, our findings for paradoxical reasoning differ quite markedly between UK and US. In the US, paradoxical reasoning was successful and proved more effective than the video intervention in shifting our primary outcome variable, namely the subjects’ vaccination intentions. In contrast, in the UK, we found no evidence that paradoxical reasoning can be a helpful tool to combat vaccine hesitancy. If anything, the evidence we obtain in our UK sample points in the opposite direction: exposure to paradoxical reasoning may worsen vaccine perceptions. We believe that a possible rationale for this discrepancy lies in the different makeup of vaccine-hesitant populations in US and UK. In the US, the public discourse surrounding vaccinations is heavily fractured around political lines. with the result that people’ s positions on vaccination are often politically motivated. This process of fictionalisation was also evident among our subjects. We used the subjects’ expressed concerns over side effects and their reaction to simple information to construct a measure of “motivated beliefs”, capturing the (conscious or unconscious) tendency of individuals to form ad-hoc beliefs that justify remaining unvaccinated. Compared to Democrats, we find that Republican and Independent score significantly higher in our motivated reasoning index. Among our UK subjects, in contrast, the tendency to engage in motivated reasoning seems to be independent of political affiliation, possibly reflecting the fact that, in the UK political arena, we do not observe the same type of political fictionalisation on matters surrounding vaccination as we do in the US.
Another notable feature is that, in the US, we observe very clear geographic patterns in our subjects’ attitudes towards the vaccine, with people living in rural areas, in particular the rural West, expressing considerably more negative attitudes. Geographic patterns also emerge in the UK (for instance, subjects located in the North tend to hold more negative vaccine attitudes compared to those in the South) but they are less pronounced.
The result that paradoxical reasoning can successfully penetrate the resistance of politically motivated vaccine-hesitant populations is a very remarkable finding in its own right. It points to the idea that unorthodox circumstances may require unorthodox interventions, and that sometimes, to induce individuals to see the logical fallacies in their positions, the most effective approach may be to embrace their views, bringing them to their extreme consequences.
We are now in the process of disseminating our findings among stakeholders and healthcare professionals. While our video interventions are relatively straightforward to implement, paradoxical reasoning could be more challenging, due to its very provocative nature. We are currently devoting our efforts to discussing possible implementation methods with healthcare providers and policy-makers.
References
The Atlantic (July 2021) “Vaccination in America Might Have Only One Tragic Path Forward.”. Bénabou, R. (2015) “The economics of motivated beliefs.” Revue d’économie politique, 125(5).
Bump, P. (2021) “Comparing the Red-State Pandemic Response Now to Blue States in EARLY 2020 Is Dishonest.” The Washington Post. https://www.washingtonpost.com/politics/2021/08/31/comparing-red-state- pandemic-response-now-blue-states-early-2020-is-dishonest/.
Dubé, E., Vivion, M., & MacDonald, N. E. (2015). Vaccine hesitancy, vaccine refusal and the anti-vaccine movement: influence, impact and implications. Expert review of vaccines, 14(1).
Hameiri, B., Nabet, E., Bar-Tal, D., & Halperin, E. (2018). “Paradoxical thinking as a conflict-resolution intervention: Comparison to alternative interventions and examination of psychological mechanisms.” Personality and Social Psychology Bulletin, 44(1), 122-139.
Johns Hopkins Center for Communication Programs “Covid Behaviors Dashboard.” https://covidbehaviors.org/.
Kahan, D.M. (2015) “The politically motivated reasoning paradigm,” Emerging Trends in Social Behavioral Sciences.
Kates, J., Tolbert, J. and Orgera, K. (2021) “The Red/Blue Divide in COVID-19 Vaccination Rates” available at https://www.kff.org/policy-watch/the-red-blue-divide-in-covid-19-vaccination-rates/
Klymak, M. and Vlandas, T. (2020) “COVID-19 Partisanship in the UK: Findings from Survey and Mobility Data”, mimeo, University of Oxford.
Klymak, M. and Vlandas, T. (2021) “Vaccination and partisanship during COVID-19 in England”, mimeo, University of Oxford.
The New York Times. “See How Vaccinations Are Going in Your County and State.” https://www.nytimes.com/ interactive/2020/us/covid-19-vaccine-doses.html.
Nyhan, B., Reifler, J., Richey, S., and Freed, G. L. (2014) “Effective messages in vaccine promotion: a randomized trial.” Pediatrics, 133(4)
Nyhan, B., and Reifler J. (2015) “Displacing misinformation about events: An experimental test of causal corrections.” Journal of Experimental Political Science 2(1).
Opel, D. J., Heritage, J., Taylor, J. A., Mangione-Smith, R., Salas, H. S., DeVere, V., Robinson, J. D. (2013). “The architecture of provider-parent vaccine discussions at health supervision visits” Pediatrics, 132(6).
Porat, T., Burnell, R. Calvo, R. A. Ford, E. Paudyal, P. Baxter, W. L. and Parush, A. (2021) “Vaccine Passports May Backfire: Findings from a Cross-Sectional Study in the UK and Israel on Willingness to Get Vaccinated against COVID-19” Vaccines 9(8).
Swann, W. B., Pelham, B. W. and Chidester, T. R. (1988) “Change through paradox: using self-verification to alter beliefs.” Journal of personality and social psychology 54(2).
Todd, C., Murray, M. and Kamisar, B. (2021) “NBC News Poll Shows Demographic Breakdown of the Vaccinated in the U.S.” NBCNews.com. NBCUniversal News Group. https://www.nbcnews.com/politics/meet-the-press / nbc-news-poll-shows-demographic-breakdown-vaccinated-u-s-n1277514.
Wilkes, A. L., and Leatherbarrow, M. (1988) “Editing episodic memory following the identification of error.” The Quarterly Journal of Experimental Psychology 40(2)
Citations
- See e.g. https://www.nhs.uk/conditions/coronavirus-covid-19/coronavirus-vaccination/safety-and-side-effects/.
- “See How Vaccinations Are Going in Your County and State.” The New York Times. December 17, 2020. https://www.nytimes.com/ interactive/2020/us/covid-19-vaccine-doses.html.
- “COVID Behaviors Dashboard - Johns Hopkins Center for Communication Programs.” https://covidbehaviors.org/.
- “Vaccination in America Might Have Only One Tragic Path Forward.” The Atlantic, July 20, 2021.
- Todd, Chuck, Mark Murray, and Ben Kamisar. “NBC News Poll Shows Demographic Breakdown of the Vaccinated in the U.S.” NBCNews.com. NBCUniversal News Group, August 24, 2021. https://www.nbcnews.com/politics/meet-the-press /nbc-news-poll- showsdemographic-breakdown-vaccinated-u-s-n1277514.
- Porat, Talya, Ryan Burnell, Rafael A. Calvo, Elizabeth Ford, Priya Paudyal, Weston L. Baxter, and Avi Parush. (2021.)”“Vaccine Passports” May Backfire: Findings from a CrossSectional Study in the UK and Israel on Willingness to Get Vaccinated against COVID-19” Vaccines 9, no. 8: 902.
- The Guardian ‘Fascist and tyrannical’: US vaccine mandates induce rightwing hysteria, 16th September 2021 https://www.theguardian. com/us-news/2021/sep/16/vaccine-mandates-rightwing-hysteria-joe-biden.
- Wilkes, A. L., and M. Leatherbarrow. (1988) “Editing episodic memory following the identification of error.” The Quarterly Journal of Experimental Psychology 40.2; Nyhan, Brendan, and Jason Reifler. (2015). “Displacing misinformation about events: An experimental test of causal corrections.” Journal of Experimental Political Science 2.1
- Swann, William B., Brett W. Pelham, and Thomas R. Chidester.” (1988) Change through paradox: using self-verification to alter beliefs.” Journal of personality and social psychology 54.2; Hameiri, Boaz, et al. (2018). “Paradoxical thinking as a conflict-resolution intervention: Comparison to alternative interventions and examination of psychological mechanisms.” Personality and Social Psychology Bulletin 44.1
- Lucid (https://luc.id/) and Prolific (https://www.prolific.co/)
- Full details including the scripts of our videos, the texts of our paradoxical interventions, the exact wording of the questions contained in our questionnaire, our order of operations and the screenshots of our experiment can be found in the long version of the report.
- Each index was constructed by taking the mean of the relevant variables, and then standardizing this mean value across subjects. Our indices thus had a mean of 0 and standard deviation of 1
- Kahan, Dan M., (2015). ‘The politically motivated reasoning paradigm’. Emerging Trends in Social Behavioral Sciences.
- See e.g. Bénabou (2015) for an overview of the economics of motivated beliefs. Bénabou, Roland, (2015). ‘The economics of motivated beliefs Revue d’économie politique, 125(5), pp.665-685.
- These findings are broadly consistent with those of other studies, see e.g. Todd, Chuck, Mark Murray, and Ben Kamisar. “NBC News Poll Shows Demographic Breakdown of the Vaccinated in the U.S.” NBCNews.com. NBCUniversal News Group, August 24, 2021. https://www. nbcnews.com/politics/meet-the-press /nbc-news-poll-showsdemographic-breakdown-vaccinated-u-s-n1277514.
- Education was measured on scale of progressively increasing level of education, featuring “no formal qualifications” at the lower end and “doctoral degree” at the upper end.
- The video optional treatment was run only in the US.
- However, we must note that we did not detect any effect of the paradoxical intervention on Perception2 and Perception3, our secondary outcome variables
- However, we must note that, in terms of changes in vaccination status, we did not find that subjects who were exposed to our treatment were more likely to have changed their vaccination status during the week following the intervention. This is possibly due to the time period elapsed (one week) being too short for any meaningful change to be observed.
Summary
- Published
© The authors. This is an open access publication licensed under a Creative Commons Attribution-NonCommercial- NoDerivs 4.0 Unported License
To cite this report: British Academy (2022), Securing the Goalposts on Vaccine Hesitancy, The British Academy, London
- DOI doi.org/10.5871/c19-recovery/S-S-A-B-G-C-S-K (Opens in a new window)