Psychological Influences on COVID-19 Preventive Behaviours and Vaccine Engagement in the USA and UK
Psychological Influences on COVID-19 Preventive Behaviours and Vaccine Engagement in the USA and UK
By Rusi Jaspal, Julie Barnett, Daniel Wright and Glynis M. Breakwell
Download PDF report
- Published by
- British Academy
- Year
- 2022
- Pages
- 19
Spanish language edition
A Spanish language edition of this summary is available.
About the authors
Professor Rusi Jaspal is Pro-Vice Chancellor and Professor of Psychology at the University of Brighton. Professor Julie Barnett is Professor of Health Psychology at the University of Bath. Professor Daniel Wright is the Dunn Family Foundation Endowed Chair and Professor of Educational Assessment at the University of Nevada, Las Vegas. Professor Dame Glynis Breakwell DBE DL is Emeritus Professor at the University of Bath and Visiting Professor at the University of Surrey and Imperial College London.
About the COVID-19 Recovery: Building Future Pandemic Preparedness and Understanding Citizen Engagement in the USA and UK
The programme is the result of a partnership between the British Academy, the Social Sciences Research Council (SSRC) and the Science & Innovation Network in the USA (SIN USA) to award funding to ten transatlantic studies focusing on UK-US COVID-19 vaccine engagement. It follows a pilot study exploring levels of vaccine engagement in four locations across the US and UK, while the larger programme was expanded to study multiple locations. The programme was funded by the UK’s Department for Business, Energy and Industrial Strategy.
Introduction
This report summarises the findings of three integrative studies conducted to examine psychological influences on citizen COVID-19 preventive behaviours and vaccine engagement in the UK and US with particular regard to the significance of ethnicity. This report focuses on the main policy implications of this research.
In section 2.0, we present a brief review of psychological research literature on ethnicity in relation to COVID-19 preventive behaviours and vaccine acceptance/ hesitancy through the lens of a social psychological framework for action analysis (Study 1). In section 3.0, we outline the results of our secondary analysis of the Imperial COVID-19 behaviour tracker multi-national data set that focuses on people’s behaviours, attitudes, and beliefs related to COVID-19 (Study 2). Section 4.0 outlines the results of our experimental study which focuses on the role of ethnicity and uncertainty on vaccination attitudes and likelihood of COVID-19 preventive behaviour and vaccination (Study 3). The relations between these three studies are illustrated in the concluding section of this summary report.
A key focus of this report is on how learning from the current pandemic might inform responses to future pandemics and, in particular, enhance our collective preparedness.
Ethnic minorities in the UK and the US
Ethnic minorities form a significant part of the UK and US population. Data from the 2011 Census show that 14% of the population in England and Wales were from ethnic minority groups and that the most populous groups were: Indians (2.5% of the population of England and Wales), Pakistanis (2%), Black Africans (1.1%) and Black Caribbeans (1.1%). According to the US Census Bureau,(1) 40% of the US population has an ethnic minority background, with 13% identifying as Black or African American; 19% as Latino; and 6% as Asian. Both the UK and the US are characterised by what Vertovec(2) calls “super diversity,” that is, “complexity surpassing anything the country has previously experienced” that is attributable to “a dynamic interplay of variables among an increased number of new, small and scattered, multiple-origin, transnationally connected, socio-economically differentiated and legally stratified immigrants.”
The significance of uncertainty
The COVID-19 pandemic has of course been characterized by much uncertainty with constantly changing rules and the contradictory messages from political and health institutions. Social identity theory suggests that situational uncertainties (such as some of those associated with vaccination) can be alleviated through identification with and active engagement in relevant, meaningful and identity enhancing (i.e., offering self-esteem, self-efficacy, positive distinctiveness and continuity) groups.(3) Mistrust is “an active state of uncertainty about whether a source or its assertions are to be believed”(4) and, as such, can lead to greater caution in accepting health advice. This mistrust can manifest in decreased trust in science and politics and is likely to be associated with lower perceived personal risk of infection, the rejection of health advice and guidance, and lower likelihood of engagement in behaviors that can decrease the risk of both infection and onward disease transmission. Mistrust that is psychologically designed for self-protection can, in practice, result in self-harm. This seems to be happening in the pattern of responses seen in some ethnic minority group members in the UK and, indeed, elsewhere.
Review of psychological research literature
Review of psychological research literature on ethnicity in relation to COVID-19 preventive behaviours and vaccine acceptance/hesitancy
In Study 1, a mapping review was conducted of the psychological research literature on ethnicity in relation to the influences determining COVID-19 preventive behaviours (including mask wearing, social distancing, social isolation, and personal hygiene) and vaccination acceptance or vaccine hesitancy.
Papers published during 2020-21 that examined psychological influences upon COVID-19 preventive behaviours (including vaccination) listed in the Web of Science or Scopus databases were identified. The initial search yielded 2198 papers, from these only those where data had been collected in either the US or UK, were published in English, reported analyses that involved ethnicity as a variable, and, examined at least one psychological correlate of one or more COVID-19 preventive behaviours were retained for analysis. Only 59 papers (i.e., 2.7%) satisfied these criteria. Thirty-two of these reported finding ethnicity effects. Few of these were based on UK data sets.
These 32 were examined to establish the levels of analysis they used to explain variations in COVID-19 preventive behaviour. Papers varied significantly in the relationships they studied. They differed in the preventive behaviour they attempted to explain. They differed in the variables whose influence they chose to explore. They rarely overlapped in the theoretical assumptions they made.
Key findings
The object of our literature review was to identify lessons emerging that are relevant to pandemic recovery and future preparedness. The lessons drawn fall into two broad domains:
- Targeting, mobilisation, and organisation of the research effort internationally and over lengthy time periods.
The research effort on the psychological variables relative to ethnicity has not been coordinated. In anticipation of future health crises, it would be advantageous to rigorously test how coordination could be mobilised across the psychological and social sciences. This will involve laying down preparatory guidelines for marshalling research resources cost-effectively in times of need. This should involve scenario planning approaches to the anticipatory design of research activities that would be required under different threat conditions. Governments and research funding agencies should commission studies now that will lay the foundations for a rapid response when the next pandemic strikes. These studies will need to be co-ordinated and international. They should build multi-disciplinary research networks that will be encouraged to continue to work together beyond single studies.
Researchers working on the social and psychological influences upon behaviour in societal crises should develop the skills to support policy-development and implementation.
- Establishing what robust evidence exists about the psychological influences underlying manifest ethnic differences in behavioural responses to COVID-19 and where the evidence is weak or absent.
The evidence base on ethnicity effects in relation to the psychological influences upon COVID-19 preventive behaviours is inadequate currently. If such research is to be used to support health intervention strategies, especially in times of crisis, a programme of work needs to be developed, in collaboration with policy makers and practitioners. The programme would involve empirical tests of intervention tactics derived from ongoing research. It would focus upon the ways change can be brought about rather than upon simply describing existing psychological determinants of health behaviours.
Broader implications
There was a concentration of effort in these papers upon psychological processes and upon social and institutional processes that shape COVID-19 preventive behaviour. There was little on the effects of sources of social influence or past action (e.g., habits).
Producing a summative map of these papers was akin to building a picture from jigsaw pieces never designed to fit together. However, some themes were evident. The most important is that the types of influences important in shaping Covid-preventive behaviours do not differ with ethnicity. For example, in relation to vaccination decisions, uncertainty about the efficacy and potentially undesirable side-effects of novel vaccines is a key factor. Ethnic groups may differ in the amount of uncertainty they report, but the significance of uncertainty is similar across groups. In addition to uncertainty, there are other types of influence that are important. Trust in the sources of information and of policy decision-making (especially in government and scientists) is a fundamental influence on COVID-19 preventive behaviour. It affects both levels of uncertainty and direction of behavioural choices. Fear of COVID-19 and perceived personal risk also affect behavioural decisions. Some papers showed personality traits, identity configuration and problem-solving competence have a role to play. This dynamic set of processes that shape COVID-19 decisions only predict actual action if the opportunity to act is present. Self-isolation may be the intention but might not be viable in crowded, shared, intergenerational accommodation.
There is nothing in the papers reviewed that suggests that the structure of the system of influences affecting COVID-19 decisions differs between ethnic groups. There is no evidence that different explanatory models are needed across ethnic groups. However, there is evidence that ethnic groups do vary on the key parameters (e.g., levels of trust, who is trusted, perceived personal risk, levels of uncertainty or scepticism, etc.) of these models.
Secondary analysis of the Imperial Data Hub COVID-19 DataHub
Building upon the findings of the Study 2, Study 3 focuses on the relationship between psychological constructs (e.g., attitudes towards vaccines) and behavioural constructs (e.g., washing hands, avoiding crowds), with emphasis on differences between the UK and the US. The aim is to understand how to measure effectively behaviours that are known to prevent the spread of COVID-19. In this part of the project we examine two aspects of this, mostly through secondary analysis of surveys from the Imperial Data Hub(5) from thirty countries. We address two issues. The first stresses that how you ask people questions in surveys affects how they answer, and therefore the estimates of people’s behaviours. If these estimates are inaccurate that affects the accuracy of the resulting epidemiological models that inform policy makers’ decisions. The second issue looks at the relationships between the psychological and behavioural constructs related to COVID-19 across many countries. Because our focus is on UK v US differences, it is important to show how these differences compare with psychological and behavioural constructs elsewhere.
Key findings
- Scepticism is important for interpreting all data, including those from surveys. The choice of response alternatives can affect how people respond and this can affect the estimates of the behaviours. This should be taken into account when constructing epidemiological models and when evaluating their precision when making policies.
- The relationship between psychological concern and adherence to health behaviours is relatively small but positive. Modelling risk behaviour requires more complex models that take into account social psychological theory.
Methodological issue: the choice of response alternatives
The Imperial Data Hub (n = 646,177 for these analyses) is being used by many researchers. Responses to all surveys question involve some measurement error based on how the questions are asked. How a question is asked can affect how it is answered, and the goal of survey designers is to ask the question such that this error as small as possible. Survey questions have two main parts: the question stem and the response alternatives. For example,
- question stem: Are you happy today?
- response alternatives: Yes/ No/ Maybe
Our focus is on how the choice of response alternatives can affect estimates of the behaviours. Because these estimates are used in epidemiological models that inform public policy, inaccurate estimates will affect the value of these models. Therefore, if questions with large measurement error are used this may negatively affect policy.
Different types of response alternatives can be used to produce behavioural estimates, but here we focus on two types: vague quantifiers and numeric categories. Consider a question such as ‘How often do you wash your hands on a typical day?’ The vague quantifiers in the Imperial Data Hub are:
Always/ Frequently/ Sometimes/ Rarely/ Not at all
The concern is whether “sometimes” means the same to different people and if there are systematic differences among countries. If people in two countries wash their hands with similar true frequencies, but have different interpretations of these, then an illusory difference may appear. In our first study using this DataHub, we split the data in two. First. we estimated the true frequency using a free-response question from another part of the survey that asks for a frequency of hand washing for part of the sample. We used the countrywide differences in these and hypothesised that these would predict differences in how people for the other part of the sample interpreted the vague quantifiers. Those in countries where hand washing frequency is high, “sometimes” corresponded to a greater frequency than for those in countries where hand washing frequency is low. Over 95% of the variation among countries in the interpretation of these vague quantifiers could be accounted for by the mean frequency estimates from the free response question answered by other respondents.
This is problematic if the goal is to estimate the behaviour. An alternative is to present a set of numeric frequency categories. We conducted a study (final n = 641) where we asked respondents several behavioural frequency questions either with a set of response alternatives concentrated at low frequencies or with a set concentrated at high frequencies. For hand washing:
The way that these sets are designed means the sum of the first three response alternatives for the low group provides an estimate for the number washing their hands three times or less. Similarly, the sum of responses for the final three categories for the high condition can be used to estimate the number washing their hands seven times or more. This allows the responses to be compared across the two conditions. Our findings show that you get higher behavioural frequency estimates if you provide respondents with numeric response alternatives that focus on high frequencies. Combined these studies show that the choice of response alternatives can affect how people answer survey questions and therefore affect the results from epidemiological models that use this information, and therefore affect policies that are informed by these models.
Psychological constructs and behaviours by country
In this section we examine the relationship between a set of questions asking about adherence to a set of behaviours and a set of questions about psychological well- being for the Imperial Data Hub. The focus is on how these vary by country and within countries by gender and age. Overall measures for psychological concerns related to COVID-19 and for following behavioural recommendations were created.
The relationship between these constructs were estimated for each of the thirty countries. The associations were small, some positive and some negative, with the average association near zero. This was surprising and shows that more involved models, like those we discuss elsewhere in this report, are necessary to model likelihood of following health recommendations with respect to COVID-19. These models can be evaluated with future pandemics.
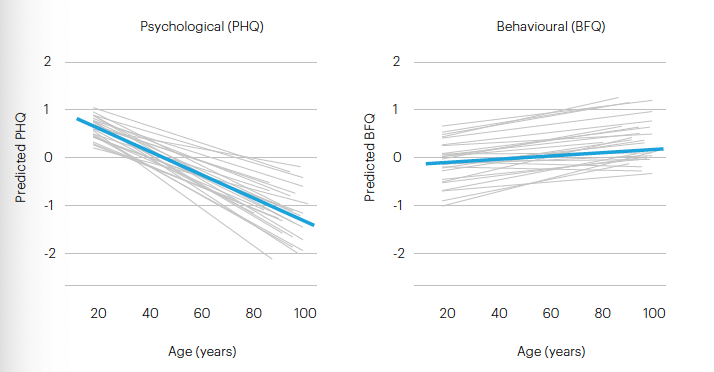
We also examined differences by demographics. Here we just consider age. Older people expressed less psychological concerns than younger people, but there was little relationship between age and following behavioural guidelines. The following figure shows the relationships for individual countries and the overall relationship. The relationship between the psychological and behavioural constructs, and age, are shown below with grey lines for each country and blue lines for the overall relationship.
Figure 1: The relationship between psychological and behavioural constructs, and age
Modelling the impact of uncertainty in an ethnically diverse sample of participants in the UK and the US
Introduction
Building on the implications of Studies 1 and 2, we designed a third study to model the impact of uncertainty in an ethnically diverse sample of participants in the UK and US. Our previous empirical studies, conducted in the UK and Portugal, have examined the relationship between a number of social psychological factors that predict willingness to engage in Covid self-protection (including mask wearing, virus testing, tracking and self-isolation) and in vaccination acceptance. Building on previous work, this study focuses on the impact of uncertainty about COVID-19 policy on vaccination attitudes and likelihood of engaging in preventive behaviour and vaccination, over and beyond identity processes, perceived risk, and mistrust. The potential causal impact of uncertainty is assessed using a quasi-experimental design. Uncertainty has been identified to be a barrier to vaccine acceptance in the context of other infectious diseases.(6) However, the role of uncertainty in relation to COVID-19 policy specifically has not been assessed. This is important especially as there has been much public uncertainty in relation to COVID-19 policy and the evolving rules and guidance relating to the pandemic. Uncertainty can induce a sense of inertia and people may disengage from things they are uncertain about as a means of protecting their identity.
Key findings
- Mistrust and uncertainty in relation to COVID-19 appear to be higher in the UK than in the US.
- On the whole, British people of Black Caribbean descent tend to report higher mistrust and uncertainty than other ethnic groups.
- Being primed to think about uncertainties in relation to COVID-19 policy is subsequently associated with more negative attitudes to their government’s performance in controlling the COVID-19 pandemic.
Methodological issues
Participants
A convenience sample of 1117 people in the UK and 763 people in the US was recruited to participate in a study of perceptions of COVID-19 prevention on Prolific, an online participant recruitment platform. There were two eligibility criteria: being aged 18 or over and being resident in either the UK or the US. Data were collected in January 2022. The following ethnic groups were included in the UK arm of the study: White, South Asian, Black Caribbean, and Black African; and the following ethnic groups in the US arm: White, Hispanic/Latino, African American, Asian.
Procedure
The study was administered and completed using Qualtrics. Participants completed baseline measures of trust in science and scientists, suspicion about information on new variants, general conspiracy theorising, fear of COVID-19, current engagement in preventive behaviour. They were then randomly allocated to one of the following three experimental conditions: (1) the uncertainty about COVID-19 policy condition, in which they were asked to think about and list five things that confused them about government policy; (2) the certainty about COVID-19 policy condition, in which they were asked to think about and list five things that made sense to them about government policy; or (3) the control condition, in which participants completed an identical questionnaire with no task to prime them to be uncertain or certain. They then completed measures of perceived risk of COVID-19, belief in the national health system to cope with the pandemic, likelihood of future COVID-19 preventive behaviour, vaccination likelihood, booster uptake likelihood, and attitudes towards anti-vaxxers, and life satisfaction.
Key results
Differences by country (UK vs. US) in the key variables of interest
In comparison to UK participants, US participants reported higher trust in science and scientists, less suspicion about information on new variants, less general conspiracy theorising, greater fear of COVID-19, less belief in the ability of the national health system to cope with the pandemic, higher current engagement in preventive behaviour, higher likelihood of future COVID-19 preventive behaviour, higher likelihood of vaccination and uptake of booster jabs, less favourable attitudes towards anti-vaxxers, and lower life satisfaction. There were no differences in perceived risk of COVID-19 between the samples. The potential interactions between the effects of country and the experimental condition on post-manipulation variables require further examination.
Differences by ethnic group in the UK
Results showed that White participants reported the most trust in science and scientists and that Black Caribbeans reported the least trust; that South Asians reported the least suspicion about information on new variants and that Black Caribbeans reported the most suspicion; that White participants reported the least general conspiracy theorising and that Black Caribbeans reported the most general conspiracy theorising; that Black Africans reported the least fear of COVID-19 and that South Asians reported the most fear; that South Asians reported the highest current engagement in preventive behaviours and that White participants reported the least current engagement; that White participants perceived themselves to be at highest risk of COVID-19 and that Black African reported the least risk; that mixed participants were less likely to believe their national health system capable of coping with the pandemic and that White participants believed it most capable; that White participants reported greater likelihood of future preventive behaviour and that Black Caribbeans reported lowest likelihood; that White participants reported highest likelihood of vaccination and of a booster jab and that Black Caribbeans reported lowest likelihood; that South Asians reported least favourable attitudes towards anti- vaxxers and that Black Caribbeans reported the most favourable attitudes; and that mixed participants reported the highest life satisfaction and that Black Caribbeans reported the lowest life satisfaction. The potential interactions between the effects of ethnic grouping and the experimental condition on post-manipulation variables require further examination.
Differences by ethnic group in the US
Results showed that African Americans reported the lowest perceived risk of COVID-19 and White participants the highest; that African Americans reported the lowest likelihood of vaccination and having a booster jab while White participants reported the highest likelihood; that White participants reported the least favourable assessment of their government’s performance in controlling the pandemic while Hispanics reported the most favourable assessment; that White respondents reported the least likelihood of engaging in preventive behaviour while African Americans reported the highest likelihood; that African Americans respondents reported the most favourable attitudes towards anti-vaxxers while Asians reported the least favourable attitudes; that African Americans reported the lowest trust in science and that Asians reported the highest trust in science; that African Americans reported the highest suspicion about novel variants while Asians reported the least suspicion; that African Americans reported the highest conspiracy theorising while Asians reported the least; and that Asians reported the highest engagement with current COVID-19 prevention and White participants the lowest. It should be noted, the potential interactions between the effects of country and the experimental condition on post- manipulation variables require further examination.
Impact of the experimental condition (certainty vs. uncertainty vs. control) on key variables of interest
The results show that participants in the uncertainty condition reported a less favourable assessment of their government’s response to the pandemic compared to the certainty condition, and that participants in the certainty condition reported a more favourable assessment of their government’s response to the pandemic than in the control condition. There were no differences on the other variables.
Discussion and key recommendations for policymakers
Key points and recommendations
- Many studies report ethnic differences in patterns of COVID-19 preventive behaviours. Very few psychological studies report analysing ethnicity effects on the factors influencing such behaviours.
- The limited evidence available suggests that the same types of influence are at work irrespective of ethnicity. It is necessary now to test how these influences differ in their effects across ethnic groups.
- The key factors influencing COVID-19 preventive behaviours (including vaccination) lie at different levels of analysis and interact with each other, they include uncertainty about the cost-benefit of action; trust/mistrust in information and decision-makers; perceived risk; pro-social motives (e.g., altruism); fear; personality and identity configuration; problem-solving ability; available social support; normative pressure; institutional and interpersonal affordances; social representational and ideological exposure; and socio-historical or environmental context.
- The research effort on the psychological variables relative to ethnicity has not been coordinated. In anticipation of future health crises, it would be advantageous to rigorously test how coordination could be mobilized. This will involve laying down preparatory guidelines for, in the future, marshalling research resources cost-effectively. This should involve scenario planning approaches anticipating designs of research activities that would be required under different threat conditions.
- Governments and research funding agencies should commission studies now that will lay the foundations for a rapid response when the next pandemic strikes. These studies will need to be co-ordinated and international. They should build multi-disciplinary research networks that will be encouraged to continue to work together beyond single studies.
- Researchers working on the social and psychological influences upon behaviour in societal crises should be incentivised to learn how to support policy-development.
- Scepticism is important for interpreting all data, including those from surveys. The choice of response alternatives can affect how people respond and this can affect the estimates of the behaviours. This should be taken into account when constructing epidemiological models and when evaluating their precision.
- In existing research, the relationship between psychological concern and adherence to health behaviours is relatively small but positive. Modelling risk behaviour requires more complex models that take into account social psychological theory.
- Mistrust and uncertainty concerning COVID-19 are higher in the UK than in the US. In both US and UK interventions to tackle mistrust and uncertainty are necessary.
- On the whole, British people of Black Caribbean descent tend to report higher mistrust and uncertainty than other ethnic groups. This suggests that targeted, culturally specific approaches to uncertainty reduction may be valuable. Working with community members to redress mistrust and uncertainty is a long-term task.
- Being primed to think about uncertainties in relation to COVID-19 policy is associated with people evaluating their government’s performance in controlling the COVID-19 pandemic more negatively in both the UK and US. This would suggest that providing individuals with opportunities to actively consider or discuss with others the definite and effective impacts of government policy would improve their confidence in their own and their government’s capacity to cope with the pandemic. The effects of such information framing would be enhanced by better science education and inculcation of trust in science.
Broader context
Our review of the psychological literature revealed that few papers examine ethnic differences in the predictors of COVID-19 preventive behaviour or vaccination likelihood and that existing analyses incorporating ethnic differences were sometimes inconclusive. Furthermore, the research we reviewed often attempted to provide explanations of COVID-19 behaviours across levels of analysis (i.e., linking the intra-psychic to interpersonal, to intra-group, to intergroup, and, to societal, which will be key to providing effective recommendations for policy makers.
Adopting a cognitive and social psychological perspective that focuses on the processes respondents use to answer questions, called cognitive aspects of survey methodology, we show that COVID-19 research findings in the social sciences should be viewed within a particular methodological context - respondents extract information implied in the response alternatives, coupled with their own expectations, and answer questions using what they feel is the appropriate amount of information. This means that responses should be viewed with caution and that we must acknowledge the limitations of self-report data in social sciences research into COVID-19. Our review showed that there could be more coordination between researchers. In anticipation of future health crises, it will be necessary to test how coordination could be mobilized. This may involve laying down preparatory guidelines for, in the future, marshalling research resources cost-effectively.
In view of the disproportionate risk of infection faced by ethnic minorities, for policy development it is important to establish the factors particularly influencing vaccination hesitancy or mistrust and denial in diverse ethnic minority communities both now and as the vaccine roll out continues in the future. The problem should not be seen as one that is only relevant during the crisis of the current pandemic. Rather, it has significant long-term implications for any vaccination regime, such as the administering of the second doses of the COVID-19 vaccines and regular vaccination updates needed against future variants of the virus. Changes in hesitancy are ongoing and the factors influencing them must be studied. It is imperative that ongoing monitoring of changes in vaccine hesitancy is conducted, particularly across sub-groups of ethnic minorities.
Our research shows the significance of uncertainty in influencing attitudes towards the government’s performance in controlling the COVID-19 pandemic with higher uncertainty leading to a poorer assessment. The social psychological antecedents of decreased trust are complex.7 It is possible that this in turn may undermine trust in authorities.
Building upon Studies 1 and 2, we conducted a third study to examine preventive behaviour in ethnic minorities in the UK and US. We found that British people of Black Caribbean descent and African Americans appear to be less trusting and to report higher uncertainty. In ethnic minorities, mistrust of authorities, including health authorities, is at least partly associated with socio-historical factors, including past and present and anticipated future experiences of prejudice and discrimination on the basis of valued identities (e.g., ethnicity, religion). This may also increase the likelihood of accepting conspiracy theories, as demonstrated not only in the context of COVID-19 but other disease outbreaks in the UK and US.8 A key mission will be to continue to promote public engagement with science and, crucially, understanding and trust of science, especially in ethnic minorities. This may in turn enhance perception of ingroup power among ethnic minorities, which has been found to influence likelihood of COVID-19 preventive behaviours.
References
Breakwell, G. M. (2020), ‘Mistrust, uncertainty and health risks’, Contemporary Social Science, 15, pp. 504. https://doi.org/10.1080/21582041.2020.1804070
Breakwell, G. M. (2021). Mistrust. Cambridge: Cambridge University Press.
Breakwell, G. M., and Jaspal, R. (2021), ‘Identity change, uncertainty and mistrust in relation to fear and risk of COVID-19’, Journal of Risk Research, 24, pp. 335-351. https://doi.org/10.1080/13669877.2020.1864011
Hogg, M. A. (2000), ‘Subjective uncertainty reduction through self-categorization: A motivational theory of social identity processes’, European Review of Social Psychology, 11, pp. 223-255. https://doi. org/10.1080/14792772043000040
Jaiswal, J., Singer, S. N., Siegel, K. and Lekas, H. (2019), ‘HIV-related ‘conspiracy beliefs’: lived experiences of racism and socio-economic exclusion among people living with HIV in New York City’, Culture, Health and Sexuality, 21, pp. 373-383. https://doi.org/10.1080/13691058.2018.1470674
Vertovec, S. (2007), ‘Super-diversity and its implications’, Ethnic and Racial Studies, 30, pp. 1024-1054. https:// doi.org/10.1080/01419870701599465
Citations
- United States Census Bureau https://www.census.gov/quickfacts/fact/table/US/PST045221
- Vertovec, S. (2007), ‘Super-diversity and its implications’, Ethnic and Racial Studies, 30, pp. 1024-1054. https://doi. org/10.1080/01419870701599465
- Hogg, M. A. (2000), ‘Subjective uncertainty reduction through self-categorization: A motivational theory of social identity processes’, European Review of Social Psychology, 11, pp. 223-255. https://doi.org/10.1080/14792772043000040
- Breakwell, G. M. (2020), ‘Mistrust, uncertainty and health risks’, Contemporary Social Science, 15, pp. 504. https://doi.org/10.1080/2158204.2020.1804070
- Imperial College London YouGov COVID-19 Behaviour Tracker Data Hub https://github.com/YouGov-Data/covid-19-tracker
- Breakwell, G. M., and Jaspal, R. (2021), ‘Identity change, uncertainty and mistrust in relation to fear and risk of COVID-19’, Journal of Risk Research, 24, pp. 335-351. https://doi.org/10.1080/13669877.2020.1864011
Summary
- Published
© The authors. This is an open access publication licensed under a Creative Commons Attribution-NonCommercial- NoDerivs 4.0 Unported License
To cite this report: British Academy (2022), Psychological Influences on COVID-19 Preventive Behaviours and Vaccine Engagement in the USA and UK, The British Academy, London
- DOI doi.org/10.5871/c19-recovery/R-J-J-B-D-W-G-B (Opens in a new window)