Overcoming Barriers to Vaccination by Empowering Citizens to Make Deliberate Choices
COVID-19 Recovery: Building Future Pandemic Preparedness and Understanding Citizen Engagement in the USA and UK
By Peter John, Peter John Loewen, Manu Savani, Brendan Nyha, John McAndrews, Sanchayan Banerjee, Richard Koenig and Blake Lee-Whiting
Download PDF report
- Published by
- British Academy
- Year
- 2022
- Pages
- 18
About the authors
Professor Peter John is Head of the School of Politics and Economics and Professor of Public Policy at King’s College London. Professor Peter John Loewen is Director of the Munk School of Global Affairs & Public Policy and a Professor in the Department of Political Science at the University of Toronto. Professor Brendan Nyhan is James O. Freedman Presidential Professor in the Department of Government at Dartmouth College. Dr John McAndrews is a research associate and managing director of the Policy, Elections, and Representation Lab (PEARL) in the Munk School of Global Affairs and Public Policy at the University of Toronto. Dr Manu Savani is a lecturer in Behavioural Public Policy at Brunel University, London. Blake Lee-Whiting is a PhD candidate in the Department of Political Science at the University of Toronto. Dr Sanchayan Banerjee is a doctoral researcher in behavioural and environmental economics at the London School of Economics and Political Science. Richard Koenig is a research student at King’s College London.
This research builds on an international collaborative effort across King’s College London, Brunel University London, the LSE, the University of Toronto, and Dartmouth College. Design and delivery of the research is thanks to a tremendous team effort from all members (in alphabetical order): Sanchayan Banerjee, Peter John, Richard Koenig, Blake Lee-Whiting, Peter John Loewen, John McAndrews, Brendan Nyhan, and Manu Savani.
The authors would like to acknowledge the excellent work of the PEARL lab in Toronto; support from the LSE behavioural economics lab; and data collection by Dynata. They would also like to express their gratitude for outstanding research assistance from Jonta Kamara, Lucia Letsch, Celine Mano, and Bea Thomson. For enquiries or further information please contact [email protected] or [email protected].
Acknowledgements
The authors are grateful to the British Academy for this opportunity and generous funding, with particular thanks to Flora Langley and Hugo Clarke for their guidance throughout the project. The authors appreciate the comments and suggestions of an anonymous peer reviewer on earlier work.
About the COVID-19 Recovery: Building Future Pandemic Preparedness and Understanding Citizen Engagement in the USA and UK
The programme is the result of a partnership between the British Academy, the Social Sciences Research Council (SSRC) and the Science & Innovation Network in the USA (SIN USA) to award funding to ten transatlantic studies focusing on UK-US COVID-19 vaccine engagement. It follows a pilot study exploring levels of vaccine engagement in four locations across the US and UK, while the larger programme was expanded to study multiple locations. The programme was funded by the UK’s Department for Business, Energy and Industrial Strategy.
Introduction
We are moving into a new phase of the COVID-19 pandemic. Two years on from the first policy measures that were implemented to contain the virus, we are searching for ‘COVID-normal’. The development of COVID-19 vaccines makes it possible now for citizens to learn to adapt to the virus. While the rollout of vaccines was the game-changer, across the G7 we see levels of public resistance both to taking the vaccination at all, and to taking up boosters. To be able to live with COVID while pursuing social and economic prosperity, the challenge is to maintain energetic and effective vaccine engagement strategies, when public interest may be moving to other issues now that the regulations around COVID are being relaxed.
Our research investigates the nature of vaccine engagement strategies employed from December 2020 to February 2022. This report summarises key findings from three timely exercises:
- A policy mapping of vaccine engagement strategies across the G7;
- A cross-country survey of over 23,000 people in the G7 countries; and
- Three large-scale survey experiments that test whether persuasive policy measures including nudges can change attitudes and intentions to take up COVID-19 vaccines and boosters
For more detailed discussion of methodology, data, and results, please see the accompanying Final Report for the research project.
Vaccine engagement across the G7
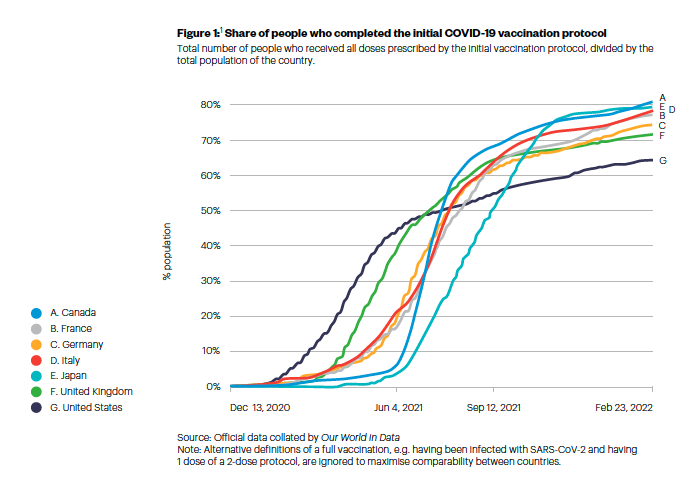
Vaccination uptake accelerated in all G7 nations during early 2021, followed by a slowing down from Summer 2021 (see Figure 1). While the number of vaccine doses administered increased during the winter of 2021/22, very likely linked to the new risks of infection that the Omicron-variant posed, the share of the population who are fully vaccinated remains below 85% (as of 23 February 2022, see Figure 2).
Canada leads the way with 81% of people having completed the initial vaccination protocol. The UK was briefly ahead among the G7 nations during July 2021; but with uptake showing signs of slowing since September 2021, the UK now reports the sixth lowest full vaccination rate of the G7. The UK, with 72% fully vaccinated, is ahead of the United States only, which lags considerably at 65%.
Figure 1:(1) Share of people who completed the initial COVID-19 vaccination protocol
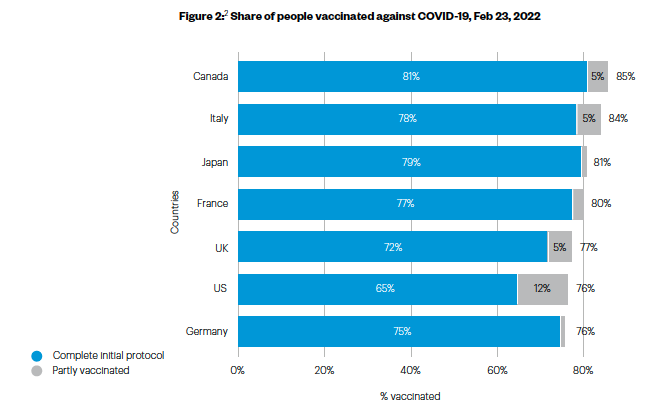
The success of vaccination efforts across the G7 deserves praise. But, as Figure 2 shows, there is more to be done. In our survey, which is representative of the populations in G7 countries, we find that 13% of people remain unvaccinated. The vast majority of the unvaccinated say they did not want to receive the vaccine (87%). People who have still not received any COVID-19 vaccination are becoming harder to reach and to persuade. Attention is growing for younger age groups too, as vaccination eligibility is expanded to include children of younger ages. Policy-makers now need to address the dual goals of encouraging people to take up the vaccine for themselves and their children.
Figure 2:(2) Share of people vaccinated against COVID-19, Feb 23, 2022
Policies used to promote vaccine engagement
G7 governments have approached vaccine rollouts with energy and pace. With the sheer range of initiatives to enable and encourage vaccine take-up, it is timely to take stock of what has been carried out and identify lessons for future policy. We synthesised policy actions across the G7 taken or announced from December 2020 to February 2022.
Our policy mapping exercise shows that:
- Three broad policy types have been used to promote vaccine engagement. These are (1) rules, laws and mandates; (2) incentives; and (3) measures to inform and persuade people, and improve the accessibility of the vaccine. The G7 nations have made use of all these policy instruments to varying degrees.
- A common example of a vaccine mandate is a Covid pass demonstrating proof of vaccination. This has incentivised vaccine take-up and, in many countries, remains crucial for leading a Covid-normal life, such as accessing public spaces and transport, and continuing to work in some sectors. Stronger mandates have been applied in some countries, which target key sectors such as healthcare or education, and people of certain age groups (such as the over-50s in Italy).
- Financial incentives have been implemented in some places, often localised and small-scale interventions. These range from the nominal (such as rewards in kind for showing proof of vaccination) to more significant (including holidays, scholarships, and large lottery cash prizes). Vaccines have been made available without user fees.
- The accessibility of vaccines has been supported through a range of measures. Mass vaccination centres, drop-in vaccination centres which do not require any appointment, and the expansion of vaccine providers across healthcare centres have all aimed to overcome practical barriers and change the choice architecture for vaccination decisions.
- National and local information campaigns and public health messaging have underpinned government policies in successive phases of the pandemic. A range of strategies have been drawn upon, often appealing to humour and emotions such as fear, as well as emphasising solidarity and the need for collective action. Campaigns have made use of key ‘messengers’ for public health advice, allowing for more tailored targeting of vulnerable groups and those who are more hesitant about vaccinations.
Harder and softer vaccine engagement approaches
All policy initiatives aim to change public behaviour, in pursuit of policy goals. Different policy actions involve different levels of coercion, and place different degrees of obligation on the individual to take notice and act accordingly. Policies that require less from the public, relying more on persuasion, have been described as ‘softer’, while those that mandate action are ‘harder’.
G7 countries can be divided into two broad groups: those that have favoured harder or softer policy approaches. Canada, France, Germany, and Italy belong to the group favouring harder policy approaches. These countries have introduced nation and sector-wide mandates, employed strict rules around vaccination status to access public venues, and with rules tightening further recently. Japan, the UK, and the US are in the group favouring softer policy approaches. These countries do not use nation-wide mandates, have less strict rules linking vaccination status to access to public spaces, and now show signs of relaxing these rules.
The G7 countries taking harder approaches have higher vaccination rates on average, and lower shares of the population who are unvaccinated (see Table 1). There are also differences in some attitudes, for example when asked about the balance between saving lives and preserving personal autonomy, people in countries with a harder policy approach were more likely to agree that saving lives should be prioritised.
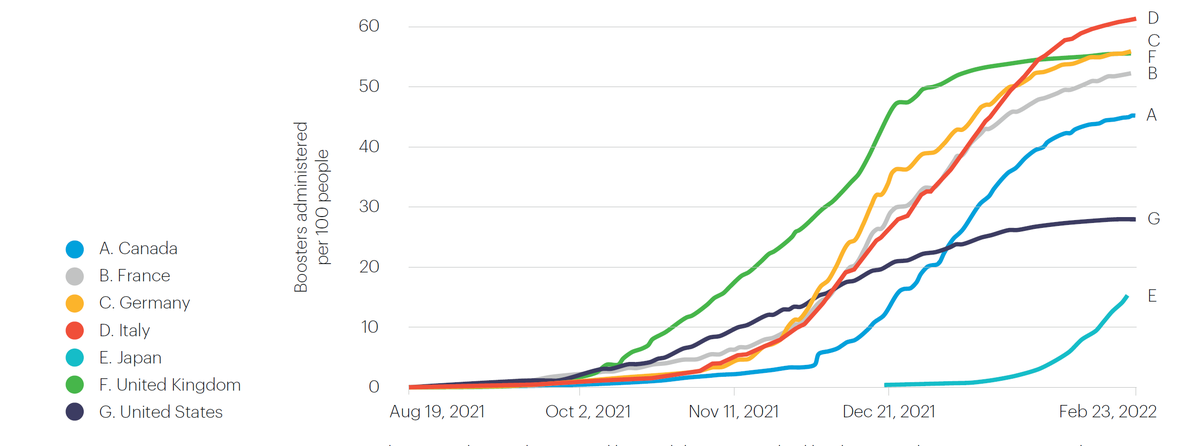
The take-up of booster vaccines is also higher in countries that favour harder policy approaches, with the US and Japan notably lagging behind the G7 (see Figure 3).
Figure 3:(3) COVID-19 vaccine boosters administered per 100 people
The distinction between hard and soft approaches is useful, but it does not directly predict vaccination engagement success. There are exceptions to the broad trends that emerge from our comparison of countries that favour harder or softer approaches. In Japan we observe a far softer policy approach than Italy, yet the share of people with a complete initial vaccine protocol are very similar (not so for boosters, however). Amongst the unvaccinated, however, those in countries with a harder policy approach are more likely to indicate vaccine refusal. It is not clear whether these attitudes are a result of the policy measures; it might also be understood as evidence of more resistant attitudes in a smaller minority of unvaccinated people.
While evidence shows a positive and significant impact of announcing and introducing vaccine mandates in some G7 countries, we are now also observing political fallout from some hard policies, such as public protests in Canada and France during February 2022. The optimal trade-off between public health and personal freedoms continues to challenge decision makers. With highly vocal and organised pockets of vaccine resistance appearing, these challenges are likely to remain for the foreseeable future and can be expected to constrain the extent to which harder vaccine engagement policies may be pursued during 2022.
Attitudes towards COVID-19 vaccines
Our survey gathers data from 23,309 respondents from across the G7 countries. The data was collected through an online survey that was fielded during January- February 2022 to all seven countries. Our dataset is a representative sample designed to approximate key socio-demographic features in each country, namely for gender, age, sub-national region, and education. It offers unique insights into people’s experiences and attitudes towards COVID-19. Further data are being collected.
We present below some compelling themes that emerge from this seven-country dataset, which relate an individual’s social, political, and demographic characteristics with their attitudes towards COVID-19 vaccines, as well as vaccination status. The relationships reported demonstrate correlation and should not be used to infer cause and effect.
Who takes up the vaccine?
- People who are fully vaccinated are likely to be aged over 35, educated to university/college level, and in full time employment. They are slightly more likely to be female (but this varies by country).
- Vaccinated respondents believe that ‘saving lives is more important than personal liberty’; and take lower levels of risk in their day to day lives.
- They are more likely to rely on conventional media than social media for news on the coronavirus.
- They are significantly more likely to trust in the vaccines, and to trust in institutions generally.
- The vaccinated are more likely to identify on the left of a left-right political scale and identify less strongly with any party they express an affiliation with.
- Vaccinated people are less likely to describe themselves as religious.
Trust
- Trust in the vaccines is reasonably high, with 78% of our survey saying that in general they trust COVID-19 vaccines. But this means nearly a fifth of residents across the G7 do not trust the vaccines. Trust in the vaccines is lowest in France (67%) and the US (71%), with Italy (85%), and the UK (85%) recording the highest levels of trust.
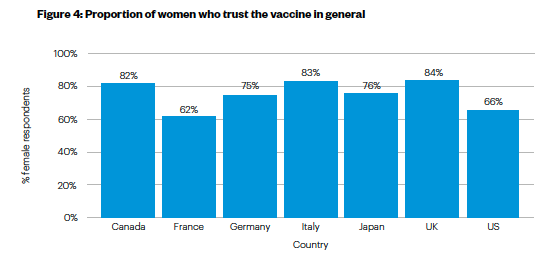
- Women trust the vaccine less than men. Across the G7, 75% of women say they trust the vaccine compared to 81% of men. Trust amongst women is lowest in France (where only 62% of women say they trust the vaccine) and the US (65%), and highest in the UK (84%).
- Most people identified public health professionals (their doctor or health care provider) as the figure they trusted the most to decide whether to have a COVID-19 vaccine or a booster. This was particularly true for older respondents (83% of those aged 65+ selected a public health messenger). Younger people were more likely than older people to choose local messengers as the figures they would trust the most (26% of 18-24-year olds).
- Being a parent appears to be slightly but negatively associated with trust in the vaccine overall. However, parents are more likely to have received at least one vaccination. Together, our findings might indicate that vaccination decisions for children require different (and more) deliberation than a vaccination decision for themselves. This warrants consideration of careful health communications for parents.
Figure 4: Proportion of women who trust the vaccine in general
Political beliefs and perceptions
- Political beliefs are significantly associated with trust in the vaccine and vaccination status.
- Those who trust the vaccine are more likely to score themselves on the left of a left-right political spectrum.
- Those who are unvaccinated are more likely to score themselves on the right of a left-right political spectrum.
- Those who believe their community is likely to be ignored by politicians are less likely to trust COVID-19 vaccines and are less likely to be vaccinated.
Media
- A large majority (81%) across the G7 used conventional sources such as radio, newspapers, and television as their primary news source on the coronavirus.
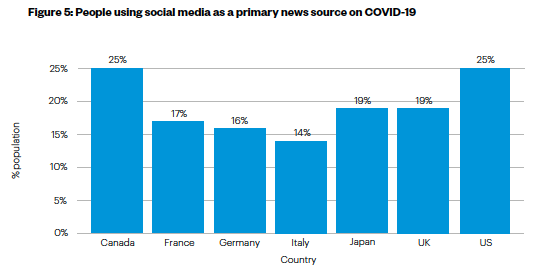
- But a sizeable minority of people relied on social media as their primary news source, including platforms like Whatsapp. This trend was more pronounced in the US and Canada (see Figure 5).
- Relying on social media as the primary source of COVID-19 news is negatively associated with vaccination status and levels of trust in the vaccine.
Figure 5: People using social media as a primary news source on COVID-19
Worry and optimism
- People worry about the side effects of the vaccine, but this varies from one country to the next. On a scale of 0 to 10, with a higher score indicating more worry, the G7 average was 4.9. France (5.7) and Italy (5.4) score high whereas the UK (4.1) and Canada (4,4) have lower levels of worry.
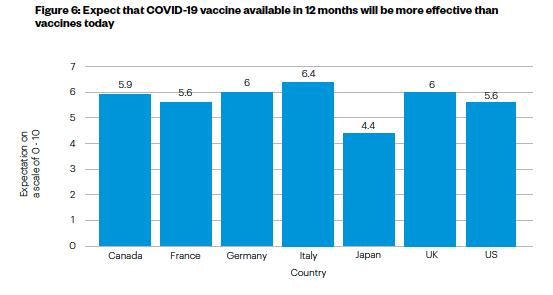
- There is considerable optimism over the potential of future vaccines. People tend to agree that COVID-19 vaccines 12 months from now will be more effective than those available today (see Figure 6). The main exception to this pattern is Japan where the average score (4.4 on a scale of 0 to 10) is lower than the G7 average (5.7), and considerably lower than in Italy (6.4), Germany and the UK (6.0).
Figure 6: Expect that COVID-19 vaccine available in 12 months will be more effective than vaccines today
Public acceptance of stringent policy
Our survey included a randomised experiment to evaluate the effect of vaccine effectiveness information on citizens’ support for policy stringency. This relationship is an important one, given the trade-off that vaccine engagement strategies have to navigate between personal autonomy and the public health protections afforded by vaccinations. In delivering public health, societies around the world have accepted new forms of government intervention in their lives, with policies that may be seen as paternalistic or even coercive.
What determines whether people will accept this intrusion that accompanies harder policy measures? We consider this question by looking at vaccine effectiveness. A more effective vaccine promises more health benefits – would this make people more likely to accept the ‘lives versus liberty’ trade-off in the form of more stringent vaccine engagement policies?
We offered hypothetical information vignettes to our survey respondent. These varied, on a random basis, the level of vaccine effectiveness from 50% to 90% (in steps of 10 percentage point). Each respondent would be informed of a particular vaccine effectiveness level. We then asked respondents whether they would support a series of policy instruments the government might use to encourage vaccination take-up: (1) making boosters freely available; (2) banning the unvaccinated from entering public spaces or using public modes of transport; (3) employer mandates for boosters; and (4) fines for the unvaccinated. These are all measures that have been announced, considered, or implemented in G7 countries.
If a respondent supported measures two, three or four, they were supporting more stringent policies. The question is whether being informed that the vaccine was less or more effective made any impact on a person’s willingness to accept hard policies such as mandates and fines. Five key findings emerge:
- Our respondents tend to favour less stringent policy. The average scores on policy support range from just over 1.5 to just under 1.6., which are reasonably low values on a scale of 0 to 4. The close clustering of scores suggests support for policy stringency does not change radically based on information about vaccine effectiveness. But some significant changes are apparent.
- A more effective vaccine leads to higher support for stringent vaccine policies, but only when vaccine effectiveness reaches a threshold value of 70% effectiveness.
- There is no additional effect on support for policy stringency beyond this threshold level of 70% effectiveness. In other words, respondents do not support stringent policies any differently when the vaccine is 80% or 90% effective – the positive effect of this information plateaus after the 70% threshold.
- Different people have different attitudes towards these stringent policies. Older adults support more stringent policies than the young; and males support more stringent policies than female. People who have already received a booster are likely to support more stringent policies than those who have not. Finally, people who said they trust the vaccine in general were likely to support more stringent policies than those who did not trust the vaccine.
- UK respondents are the least likely to support stringent vaccine policies compared to all other G7 countries, including Japan and the US which share the UK’s overall policy approach of favouring softer policies. This supports the idea that the UK’s vaccine engagement approach may be a good fit with public acceptance and attitudes on harder and softer policy measures.
In a separate experimental study, we investigated the effects of different policy measures on individuals’ support for vaccine engagement policies. We implemented a conjoint experiment, which is an increasingly common type of survey experiment that allows researchers to estimate the effects of different policy design features on individual preferences. Respondents were presented with a future scenario where the government is seeking to promote booster vaccines against new variants of COVID-19. We asked our respondents to choose between a pair of hypothetical vaccine policies. The features of the policies were randomly varied. Afterwards, participants were asked which of the two policies they preferred and how much they supported each policy. Participants repeated this task three times. Three main findings arise from this experiment:
- Policies that allowed people to schedule their own vaccine appointments increased public support, compared to policies in which a local clinic would initiate contact to schedule an appointment.
- Policies that offered people automatic reminders to get the booster also increased public support, relative to policies that offered no such reminders.
- Third, policies that included government-issued fines for eligible people who did not get the booster reduced public support - compared to policies that did not include such fines.
The prevailing message of the conjoint experiment is that people wanted governments to use a ‘light touch’ approach to managing vaccine booster policy in this hypothetical future scenario.
Nudging people to vaccinate
Nudges are widely used to promote health behaviour change, including vaccinations. They are interventions that encourage and persuade change, without altering financial incentives through fines or rewards, or mandating action through rules and regulations. The term nudge is an umbrella term for an array of different measures, from personalised text messages to commitment contracts.
We looked into how nudges can and should be designed both to improve vaccination engagement, and in a way that empowers personal choice rather than quietly bypasses it (as some nudges, like defaults, might be considered to). More deliberative approaches are often lauded for their ability to prompt deeper thought and consideration over personal decisions. Such strategies, termed ‘thinks’, have been combined with nudges in other settings, but might also serve as alternatives to nudges.
With relatively little evidence on how these design features might matter for vaccination behaviours, our question was: are nudges that incorporate some element of personal deliberation (reflection) on the health decision more effective as vaccine engagement strategies?
In a second survey experiment, we evaluated the effect of different nudge designs on two important outcomes: (1) the individual’s intentions to be vaccinated at the next opportunity, and (2) support for the vaccine policy nudge. Once again, our respondents were randomly assigned to receive an information vignette. The vignette they saw determined whether they were asked about a nudge strategy, a reflection strategy, a nudge plus reflection strategy, or a control group with no nudge. The hypothetical scenario that respondents were given involved calling their local clinic to book a booster shot. The control group received an instruction on how to do this. The nudge group were automatically enrolled to receive an appointment. The reflection group were not automatically enrolled but were asked to think about this policy for encouraging boosters. And finally, the nudge plus reflection group were automatically enrolled and asked to think about the fact that this automatic enrolment was in place.
Our findings show that the default nudge backfires, with or without reflection, compared to the status quo. Put simply, automatically scheduling booster appointments significantly reduces respondents self-reported intentions to get the booster. Yet when respondents are made to think about the nudge, their approval for the policy, relative to the standalone nudge, increases significantly by 6 percentage points. Respondents who reflect on the nudge evaluate the government’s action positively, relative to the standalone nudge scenario (even if they personally did not embrace the nudge).
Insights and lessons for the UK
Countries with a softer approach report a lower average vaccination rate in our survey. However, the UK compares favourably with the other countries (Japan and the US) that also take a softer policy approach, particularly with the booster vaccines. Unlike some countries taking a harder policy approach, the UK has not experienced the level of public protest and unrest observed in Canada and France in February 2022. The softer policy approach in the UK also seems to fit with slightly lower public agreement for prioritising lives over personal liberty. Our survey evidence highlights that trust in the vaccine remains high. The UK has thus far avoided the degree of vaccine hesitancy observed in the US. We do not see as strong a degree of vaccine refusal among women, compared to France.
What could the UK do differently in future, learning from policy experiences of other G7 countries?
Policy actions and initiatives
- As Covid rules in general grow more relaxed, for example around self-isolation and testing, the UK may want to consider the use of positive incentives to encourage ongoing vaccine uptake particularly among the young. Canada and the US display an imaginative range of incentives schemes from lotteries awarding cash prizes, to recreational activities and holidays, to educational scholarships. These are largely untested in the UK, but may hold promise.
- A number of countries have linked sporting and cultural events to vaccination campaigns, in a bid to raise and maintain the salience of the vaccine and perhaps link vaccination to freedom to enjoy life fully, and participate in national events. Anecdotal evidence suggests that these campaigns are effective, and could be particularly valuable in promoting vaccinations amongst young people.
- The second most common reason for not being vaccinated is ‘lack of time’, and this is arguably something that could be addressed through persuasive policy approaches. Nudges that remove administrative barriers and make vaccination an easier and more convenient process may more easily reach these unvaccinated people. The UK has done well to improve access to vaccines including through mass vaccination centres during 2021, an enhanced network of community pharmacies for the booster programme over 2021/22, and NHS text message communications. Borrowing from G7 countries such as Germany and Japan, the UK may want to consider extending the venues at which vaccines can be received to include other healthcare professions; and like Italy and France plan for pop-up vaccination campaigns over the summer that particularly appeal to younger age groups.
- Public expectations are important for decision makers to be aware of. 2022 promises to be a year of ongoing policy evolution as G7 countries consider the rollout, continued implementation, or rollback, of policy measures. In general, people expect Governments will recommend a further booster shot in 2022, and that vaccine passes will continue to be in use. Respondents from the UK, USA and Japan are consistently below the G7 average in these expectations, which raises questions for future public acceptance of these measures. Overall, people have optimistic expectations about vaccines but expect government controls over policy, especially in Canada, France, and Germany.
- As the ask for citizens becomes more complex after the acute period of the pandemic, we show that governments can build long-term support for nudge policies by asking citizens to think about nudges (nudge plus).
Reaching the unvaccinated
- The share of people in the UK who are unvaccinated – approximately 10% in our survey data – is relatively low in the G7, and this is welcome. The two major reasons given for not having received a vaccine yet is not wanting to, and lack of time. The direct refusal of a vaccine suggests that hesitancy may be hardening amongst a minority of people. We need to be realistic about the level of behaviour change softer policies can leverage amongst groups who actively oppose the vaccine. This resistance will not necessarily be fixed through harder policies such as mandates.
- More granular insights into anti-vaccination groups and vaccine-hesitant attitudes are needed to design effective policy. This involves a more targeted understanding and approach for people who remain unvaccinated – a group who may be more diverse than they are often portrayed as. Our survey shows that ethnic minorities should be considered carefully by sub-group. In the UK, for example, British Indians report slightly higher than average vaccination rates, while other minority ethnic groups report lower vaccination rates and may express more vaccine hesitancy. Younger people demonstrate different attitudes towards trusted messengers, which should be explored further to persuade higher uptake by the under-35s. And while parents are more likely to be vaccinated themselves, there may be lingering concerns around the vaccine for younger children, which will require targeted interventions.
Evidence
- The diverse range of policy approaches and governments’ willingness to initiate new vaccine engagement strategies lend themselves to rigorous and significant testing. The scholarly literature is catching up, but there remains a dearth of evidence investigating how effective different policy instruments have been, leaving many questions unanswered in how they should be taken forward in future.
- We need more and rigorous evidence on persuasive and informational policy tools. This could be gathered using small-scale field experiments, and would do well to move beyond the mass public to focus more carefully on specific communities that express ongoing concern and resistance to COVID-19 vaccination.
- Much could be gained from a coordinated effort to evaluate local-level interventions through randomised control trials and experimental approaches. Doing this over multiple sites allows for important lessons on how well certain interventions travel across social and political contexts. The experimental approach allows for rigorous inference of the effectiveness of a particular policy approach, such as a nudge or an incentive scheme, which will be reported on later.
- Research sustained over time, in the form of longitudinal surveys and panel research, can help improve our knowledge of vaccine engagement policies over time. This would allow us to investigate potential compliance fatigue with harder policy instruments; which policies manage to hold the public’s attention for longer; and, importantly, the evolution of attitudes amongst those who are hesitant but open to being persuaded to take a vaccine.
References
Mathieu, E., Ritchie, H., Ortiz-Ospina, E. et al. (2021) ‘A global database of COVID-19 vaccinations’. Nat Hum Behav, 5, pp. 947-953.
Our World in Data (2022) COVID-19 vaccine boosters administered per 100 people [accessed 23/02/2022].
Our World in Data (2022) Share of people who completed the initial COVID-19 vaccination protocol [accessed 23/02/2022].
Citation
- Our World in Data (2022) Share of people who completed the initial COVID-19 vaccination protocol [accessed 23/02/2022].
- Mathieu, E., Ritchie, H., Ortiz-Ospina, E. et al. (2021) ‘A global database of COVID-19 vaccinations’. Nat Hum Behav, 5, pp. 947-953.
- Our World in Data (2022) COVID-19 vaccine boosters administered per 100 people [accessed 23/02/2022].
Summary
- Published
© The authors. This is an open access publication licensed under a Creative Commons Attribution-NonCommercial- NoDerivs 4.0 Unported License
To cite this report: British Academy (2022), Overcoming barriers to vaccination by empowering citizens to make deliberate choices, The British Academy, London
- DOI doi.org/10.5871/c19-recovery/P-J-P-L-B-NJ-M-B-L-W-S-B-M-S (Opens in a new window)