Mobilised Misinformation
Addressing COVID-19 vaccine hesitancy and responding to anti-vax activism
By Reed M. Wood, Marie Juanchich, Mark Ramirez and Shenghao Zhang
Download PDF report
- Published by
- British Academy
- Year
- 2022
- Pages
- 37
About the authors
Dr Reed Wood is Reader in the Department of Government at the University of Essex. Dr Marie Juanchich is Reader in the Department of Psychology at the University of Essex. Dr Mark Ramirez is Associate Professor in the School of Politics and Global Studies at Arizona State University. Shenghao Zhang is a Ph.D. Candidate in the Department of Government at the University of Essex.
About the COVID-19 Recovery: Building Future Pandemic Preparedness and Understanding Citizen Engagement in the USA and UK Series
The programme is the result of a partnership between the British Academy, the Social Sciences Research Council (SSRC) and the Science & Innovation Network in the USA (SIN USA) to award funding to ten transatlantic studies focusing on UK-US COVID-19 vaccine engagement. It follows a pilot study exploring levels of vaccine engagement in four locations across the US and UK, while the larger programme was expanded to study multiple locations. The programme was funded by the UK’s Department for Business, Energy and Industrial Strategy.
Executive summary
The conclusions and recommendations presented in this report are based on results from two large-scale surveys conducted in the US and UK, and an experiment embedded within these surveys. The findings help advance efforts to understand and address vaccine hesitancy in several ways. First, the results demonstrate that concerns about side effects and uncertainty about vaccine efficacy remain potent predictors of vaccine hesitancy, and are at least as influential as several frequently noted socio-demographic factors. Success at reducing vaccine hesitancy will largely depend on educating reluctant individuals about the protective benefits of vaccination and ameliorating their fears about the risks of serious side effects associated with vaccination.
Second, the analyses identify a set of factors that consistently predict beliefs about vaccine safety and efficacy, including beliefs about harms to specific groups and beliefs about specific severe side effects from COVID-19 vaccines. In particular, psychological characteristics such as trust in science and government, psychological reactance, and authoritarian attitudes exert significant influence on individuals’ beliefs about COVID-19 vaccine efficacy and safety. The results suggest these characteristics might be more influential than many of the socio-demographic factors that have been the focus of much of the previous research.
Third, we conduct one of the first analyses of the factors that influence public beliefs and attitudes toward organised anti-vaccine activism. The results suggest that similar sets of factors determine beliefs about vaccine harms and affinity for anti- activism, though some important differences emerge. Unsurprisingly, unvaccinated individuals are most likely to have positive opinions of anti-vax activist groups and believe that the information these groups share is credible. Again, we find that psychological reactance and authoritarianism are influential predictors of such beliefs, and they are particularly important drivers in the US context. Political identities are also strong predictors of these attitudes in the US, while minority racial or ethnic group membership is strongly associated with affinity for anti-vax activism in the UK sample.
Fourth, we provide evidence that correction and debunking can effectively counteract vaccine inaccurate beliefs about the risks of COVID-19 vaccines. Yet, the results reveal that the source of the correction matters: debunking by health care professionals reduces belief in vaccine harms, whereas the same efforts by government or political authorities has no discernible effect on these beliefs.
However, debunking by medical professionals only altered vaccine attitudes among British respondents. Condemnation and criticism of anti-vaccine activists appears to have little effect on these beliefs, but it does not appear to result in backlash. Paired with the information from the broader survey, this result suggests that enhancing efforts to counter the myths and misinformation spread by anti-activists may help to promote confidence in COVID-19 vaccines.
These findings should be useful for policymakers and health practitioners. In particular, the report highlights the need to address the persistent fears citizens may have about the potential harms they believe to be associated with COVID-19 vaccines, to tailor messaging to these communities that recognises the psychological underpinnings of vaccine scepticism, and to counteract vaccine misinformation disseminated by anti-vaccination activists through consistent correction efforts by respected health care professionals.
List of figures
Figure 1: Structure of experiment 9
Figure 2: Correlates of receiving one or more vaccine doses 10
Figure 3: Correlates of beliefs about covid-19 vaccines 13
Figure 4: Correlates of attitudes toward anti-vaccination activism 17 (US respondents)
Figure 5: Correlates of attitudes toward anti-vaccination activism 18 (UK respondents)
Figure 6: Effects of misinformation on beliefs about group-specific harms 21
Figure 7: Effects of misinformation on beliefs about side effects 22
Figure 8: Effects of responses to misinformation on beliefs about 24 group-specific harms
Figure 9: Effects of responses to misinformation on beliefs about side effects 25
Figure A1: COVID-19 vaccination rates 31
Figure A2: Beliefs about COVID-19 vaccines 31
Figure A3: Belief in group-specific harms from COVID-19 vaccination 33
Figure A4: Belief in side effects from COVID-19 vaccination 34
Figure A5: Attitudes toward anti-vaccination activism 35
Research overview
Despite the general success of vaccination campaigns in most high-income countries, millions of adults and adolescents in the United States and the United Kingdom remain unvaccinated. Notably, vaccine hesitancy is not uniformly distributed across the populations of those countries; rather, identifiable subsets of the population, including some minority communities, individuals residing in lower income areas and those in rural and geographically remote areas, and younger adults and adolescents, demonstrate vaccination rates significantly below their countries’ national averages. Understanding the reasons for vaccine hesitancy within these groups is a central concern of public health practitioners and medical professionals. In particular, gaps in vaccine coverage expose significant numbers of citizens to infection and severe illness, which in turn contributes to persistent strain on national health systems.
The belief that vaccines often cause severe side effects represents a potent source of vaccine hesitancy, and thus serves as powerful deterrent to vaccination. Despite the extremely low numbers of severe side effects observed among the hundreds of millions of vaccine doses administered globally, a non-trivial number of individuals nonetheless remain fearful that vaccines will cause more harm than the disease they are intended to prevent or ameliorate. Problematically, individuals that hold these beliefs are significantly less likely to protect themselves from COVID-19 by accepting a vaccine against it. Consequently, convincing sceptical individuals of the safety of vaccines represents a fundamental challenge for governments and public health authorities.
Misinformation likely plays a central role in promoting and exaggerating individuals’ fears about vaccine side effects. In turn, social activism plays a central role in disseminating vaccine misinformation. Since the early days of the pandemic, organised groups of activists have intentionally spread misinformation about COVID-19 and COVID-19 vaccines. Through these efforts, anti-vax activists seek to sow uncertainty and doubt about the effectiveness of vaccines, stoke fears about the risk of harms associated with the vaccines, and promote scepticism of the authorities that develop and deliver them. Considering the role that beliefs regarding vaccine safety and efficacy play in predicting an individual’s vaccine status, anti-vax activism likely plays a significant role in reinforcing disparities in vaccine uptake. Consequently, responding to the public health threat posed by COVID-19 misinformation has become a primary concern for governments and public health authorities.
In the following report, we summarise the results of a series of inter-related studies that seek to address the issues raised above. Principally, we investigated the following:
- What role do respondent beliefs about the safety and efficacy of COVID-19 vaccines play in decisions to vaccinate?
- What factors determine beliefs about COVID-19 safety and efficacy?
- What factors determine public attitudes towards organised anti-vaccine activism?
- To what extent does exposure to anti-vaccine misinformation (through social media posts or through anti-vax protests) influence observed beliefs about vaccine safety and efficacy?
- How does the manner in which authorities respond to such information (i.e., condemnation vs. factual debunking) and the source of these responses (i.e., health authorities vs. political authorities) influence respondents’ willingness to believe anti-vaccine misinformation?
Results from a survey deployed to nearly 6000 respondents in the United States and the United Kingdom and from an experiment embedded within this survey provide insights into these issues.
Methodology
In order to address these issues, we conduct nationally representative, multi- wave surveys (n=2900) of adults in both the UK and the US, followed by a survey experiment deployed to the same respondents that took part in the initial survey. The surveys allow us to broadly identify the socio-demographic and psychological factors that influence an individual’s decision to receive a COVID-19 vaccine as well as how beliefs about vaccine risks and efficacy influence that decision. They additionally offer insights into the predictors of respondents’ beliefs about the risks of harms associated with COVID-19 vaccines as well respondents’ attitudes toward anti-vaccine activism and anti-vaccine organisations. The multi-country nature of the survey allows us to examine cross-country differences in vaccine attitudes. The experimental components of the study examine the role of anti-vax activism on respondents’ attitudes toward vaccines and beliefs about their potential to harm recipients, as well as how the manner in which experts and authorities respond to such activism influences respondents’ susceptibility to the misinformation anti-vax groups disseminate.
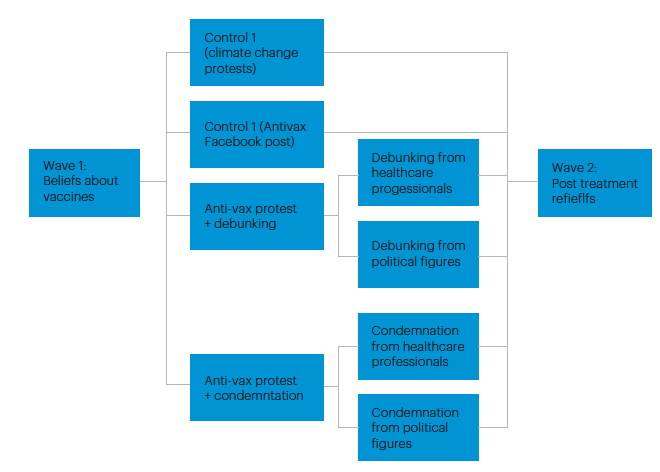
We rely on a “test-retest” between-subjects experimental protocol with a control group.(1) Wave 1 of the survey included core demographic, political, and psychological questions as well as a battery of questions probing respondents’ attitudes and beliefs about COVID-19 vaccines. Wave 2, which was deployed approximately 3 weeks later to a subset of Wave 1 respondents, included the experiment as well as the same vaccine- related questions that were administered in the first wave. This design allows us to observe whether a given condition produced an observable change in respondents’ attitudes rather than simply informing us about differences in respondents’ attitudes across different conditions.
All surveys are deployed by the survey firm YouGov, which also selects and manages the pool of respondents. The first waves of each sample include approximately 2900 adults (18 years+) respondents. YouGov provides samples that are representative of the national population based on standard demographic factors (e.g., education, age, gender, etc.). Due to the nature of this investigation and the previously reported vaccination inequalities between White and minority respondents in both countries, we oversampled respondents from minority groups. Specifically, 51% of our US sample is non-White, while 24% of our UK sample is non-White. We further oversample on parents of children under 16 years of age. Our samples comprise 28% and 26% parents of younger children in the US and UK respectively. We achieved recontact rates of over 75% in both samples, with approximately 2,300 Wave 2 respondents in the UK sample and 2,200 respondents in the US sample.(2)
An experiment embedded within our survey allows us to examine whether exposure to anti-vaccine misinformation via different channels (social media vs. organised protest) influence observer beliefs about vaccine safety and efficacy as well as the extent to which different types of responses to such misinformation (commendation vs. debunking) by different types of authorities (medical professionals vs. political authorities) can influence such beliefs. Figure 1 illustrates the structure of our experiment.
Figure 1: Structure of experiment
Beliefs about vaccine safety and efficacy as motivators of vaccine hesitancy
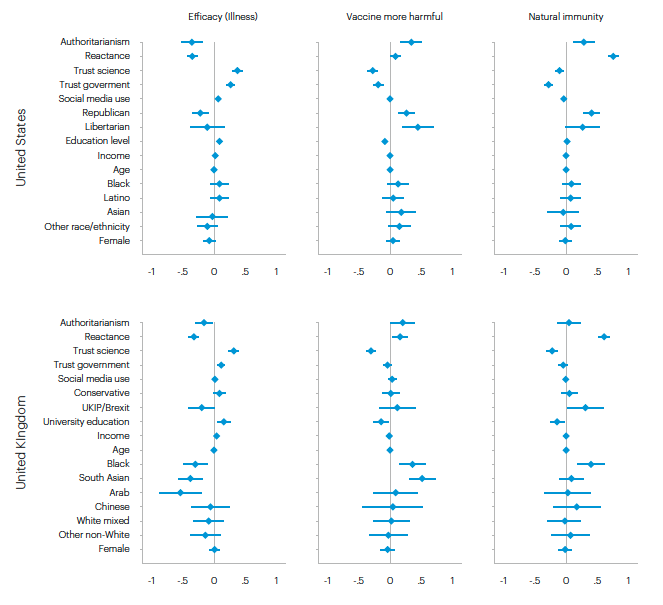
Figure 2 presents the results from a series of linear regression analyses modelling the relationship between the various indicators of vaccine hesitancy and beliefs about COVID-19 vaccines and sets of covariates, which are largely drawn from previous published studies. For ease of interpretation, we present all results as plots of coefficient estimates. In each plot, the diamond-shaped marker indicated the coefficient estimate, while the narrow horizontal lines denote 95% confidence intervals. The vertical red line located at zero on the x-axis represents the significance threshold: confidence intervals that are fully to the right or the left of the line are significant at p=0.05. Overall, the results dovetail with the results published in previous studies. However, they highlight some important differences in the predictors of vaccine hesitancy among US respondents compared to UK respondents.
Figure 2: Correlates of receiving one or more vaccine doses
We summarise our results as follows:
- Perceptions of vaccine safety and efficacy are significant and substantively meaningful predictors of vaccine hesitancy. In both the US and the UK, survey respondents that believed that a) COVID-19 vaccines are more harmful than COVID-19 infection, b) vaccines were ineffective at preventing serious illness, and c) natural immunity was superior to vaccine-acquired immunity were less likely to report being vaccinated.
- After controlling for beliefs about vaccine safety and efficacy (right-hand column of Figure 1), several factors previously linked to vaccine hesitancy become insignificant or less substantively meaningful. This includes, for example, psychological reactance, trust in science and government, Republican party affiliation (in the US), and identifying as Black (in the UK).
- This finding highlights the critical role addressing perceptions of vaccine risk and efficacy play in promoting vaccine uptake.
Factors predicting beliefs about safety and efficacy
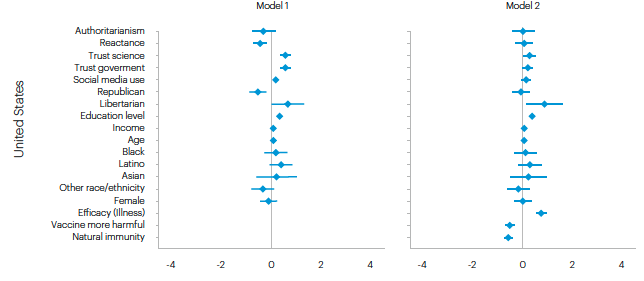
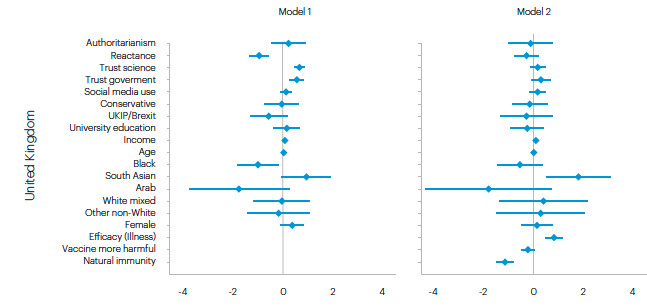
Figure 3 shows results from models predicting respondents’ beliefs about COVID-19 vaccines. These represent the three additional covariates added in the second models of the previous set of analyses (right-hand side). Given their significance and their effect on the significance of other variables in the model, it is important to understand the factors that predict these beliefs.
We summarise these results as follows:
- A variety of socio-demographic and psychological factors influence respondents’ perceptions of vaccine safety and efficacy. In general, the psychological factors predicting these beliefs are similar in the US and the UK; however, the influence of political ideology and ethnicity varies across the two samples.
- In both countries, respondents with more authoritarian attitudes and greater levels of psychological reactance(3) are more likely to express doubts about the safety and efficacy of vaccines, though the effect of authoritarian attitude is weaker in the UK sample. Similarly, in both samples, individuals with lower levels of trust in government and trust in science expressed greater scepticism regarding vaccines safety and efficacy.
- In the US, race did not appear to predict respondent beliefs about vaccine safety and efficacy. Rather, political ideology appears to be a primary driver of these beliefs: respondents identifying as Republicans or Libertarians were much more likely to express scepticism about the safety and efficacy of COID-19 vaccines.
- In the UK, political preference were not primary predictors of these beliefs, though supporters of UKIP or the Brexit Party were more sceptical of COVID-19 vaccines than other respondents. However, race and ethnicity were strongly related to beliefs about vaccine safety and efficacy. Black, Arab, and South Asian individuals were most likely to doubt that COVID-19 vaccines confirmed substantial protection from disease, while Black and South Asian individuals were more likely to express concerns about vaccine side effects.
Figure 3: Correlates of beliefs about COVID-19 vaccines
Public attitudes toward anti-vax activist groups
As we demonstrate above, the belief that vaccines often cause severe side effects represents a potent source of vaccine hesitancy, and thus serves as powerful deterrent to vaccination. Despite the very low rate of severe side effects observed among the hundreds of millions of vaccine doses administered globally, a non-trivial number of individuals nonetheless remain fearful that vaccines will cause more harm than the disease they are intended to prevent or ameliorate. Problematically, individuals that hold these beliefs are significantly less likely to protect themselves from COVID-19 by accepting a vaccine against it. Consequently, convincing sceptical individuals of the safety of vaccines represents a fundamental challenge for governments and public health authorities.
Misinformation plays a central role in promoting and exaggerating individuals’ fears about vaccine side effects. In general, members of the public possess relatively limited knowledge about the mechanisms through which vaccines protect against disease. Similarly, they have only a cursory awareness about the process of vaccine development, the rigors of drug trials, or the health and safety evaluations that most countries require prior to approving and distributing vaccines. This low knowledge environment also creates significant opportunities for the diffusion of misinformation and the perpetuation of false beliefs about vaccine efficacy and safety. In particular, individuals with low levels of trust in government and science are most susceptible to myths, false narratives, and inaccurate information about vaccines,4 which may partly explain their greater level of vaccine hesitancy.
Social activism is an important means for disseminating vaccine misinformation. Since the early days of the pandemic, organised groups of activists have intentionally spread misinformation about COVID-19 and COVID-19 vaccines. Through these efforts, anti-vax activists seek to sow uncertainty and doubt about the effectiveness of vaccines, stoke fears about the risk of harms associated with the vaccines, and promote scepticism of the authorities that develop and deliver them. Considering the role that beliefs regarding vaccine safety and efficacy play in predicting an individual’s vaccine status, anti-vax activism likely plays a significant role in reinforcing disparities in vaccine uptake.
Anti-vaccine activism predates the COVID-19 pandemic in both the US and the UK. However, the pandemic has created new opportunities for anti-vax groups to mobilise, recruit supporters, and expand their public influence. Notably, the anti-COVID-19 vaccine groups that have emerged during the pandemic differ somewhat from the broader anti-vax movement that preceded them. First, whereas the broader anti-vax movement typically expresses broad opposition to vaccines, anti-COVID-19 vaccine activism often focuses specifically on the perceived dangers of COVID-19 vaccines while remaining agnostic (or even supporting) vaccines for other diseases. This approach may lend these groups some credibility by allowing them to deflect claims that they are anti-science and by differentiating them from the broader anti- vax movement. Second, anti-COVID-19 vaccine activist groups are embedded within a larger constellation of activist groups jointly mobilised by various grievances, fears, and beliefs about the COVID-19 pandemic, which often results in significant overlap in the activities and memberships of these groups. In this sense, it is often difficult to disentangle activism directed against vaccines from activism directed against other aspects of pandemic management. The implications of these distinct features of anti-COVID-19 vaccine activism remain underexplored. However, it is likely that the narrow focus on COVID-19 vaccines—as opposed to more general vaccine scepticism—coupled with efforts to exploit uncertainty about the origins of COVID-19 and public frustrations with pandemic restrictions enhance the influence of these groups.
Anti-vax activists adopt a variety of strategies to accomplish their goals, including spreading misinformation via social media and engaging in more conventional public protest actions. Even before the COVID-19 pandemic, public health professionals, politicians, and scholars highlighted the potential threat posed to vaccination campaigns (and public health more broadly) by online misinformation disseminated via activists on social media.(5) Concerningly, recent experimental studies provide some evidence that exposure to online misinformation about COVID-19 vaccines reduces observers’ intent to vaccinate.(6) Similarly, survey data suggest that more frequent exposure to online misinformation about COVID-19 vaccines correlates with greater vaccine hesitancy.(7)
Responding to the public health threat posed by COVID-19 misinformation has become a primary concern for governments and public health authorities. In a parallel manner, systematic analyses mapping the spread of such misinformation through social networks and evaluating its impact on individual attitudes and beliefs about vaccines have increased dramatically. By comparison, there are relatively few high quality, systematic analyses evaluating the effectiveness of various strategies for counteracting myths and misinformation about the risks and efficacy of COVID-19 vaccines. Given the previously highlighted correlation between individual belief about vaccine safety and efficacy, efforts to counteract or correct misinformation and promote an accurate understanding of the risk-benefit balance of COVID-19 vaccine is critically important for promoting vaccine uptake.
While the distribution of misinformation through social media outlets has received significant attention since the start of the pandemic, it is not the only strategy anti- vax activists have utilized to promote vaccine hesitancy and scepticism. Protests targeting vaccines and vaccine mandates are increasingly common across the US and the UK. Moreover, recent clashes between anti-vax protesters and police in several countries suggest that these groups are becoming increasingly militant and adopting more hostile tactics in an attempt draw attention to their cause and pressure politicians to drop proposed vaccine mandates.8 Understanding whether these events influence observers’ attitudes towards vaccines, comparing these effects to other forms on anti-vax activism, and identifying effective strategies for responding to anti-vax activism represent important aspects of authorities’ efforts to address vaccine disparities. Like other social movement organizations, anti-vax groups routinely engage in protests and other public demonstrations. These events are intended to generate publicity for the movement, disseminate the group’s narrative, and signal the group’s strength and commitment to key audiences. By generating publicity for the movement, providing opportunities for organizations to disseminate (mis) information, and allowing groups to signal strength and resolve, protest actions by anti-vax movement organisation may play an important role in promoting vaccine scepticism. Moreover, to the extent that the narratives these events perpetuate resonate with target audiences, anti-vax protests likely reinforce observed disparities in vaccine confidence across different social groups.
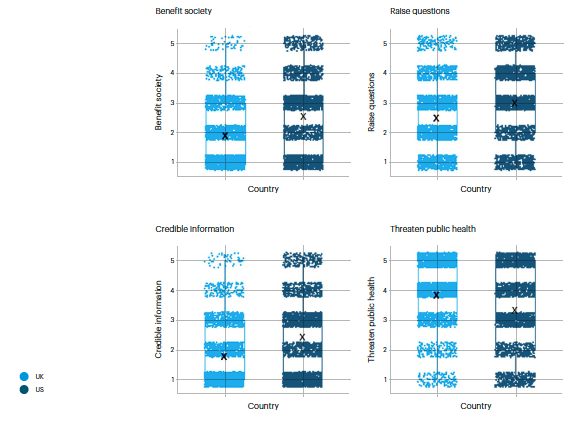
As a crucial first step in developing a more comprehensive understanding of the role that anti-vaccine activism plays in COVID-19 vaccine hesitancy, we seek to identify the factors associated with public attitudes toward organised anti-vaccine activism. In our survey, we asked respondents to indicate whether they agreed or disagreed with a series of statements about activist groups that at attempt to discourage people from getting a COVID-19 vaccine. Specifically, we asked them whether they believed such groups 1) benefit society, 2) raise important questions about COVID-19 and COVID-19 vaccines, 3), share credible information about COVID-19 and COVID-19 vaccines, and 4) threaten public health. The panels in Figures 4 and 5 show the effects of several covariates on these beliefs.
Figure 4: Correlates of attitudes toward anti-vaccination activism (US respondents)
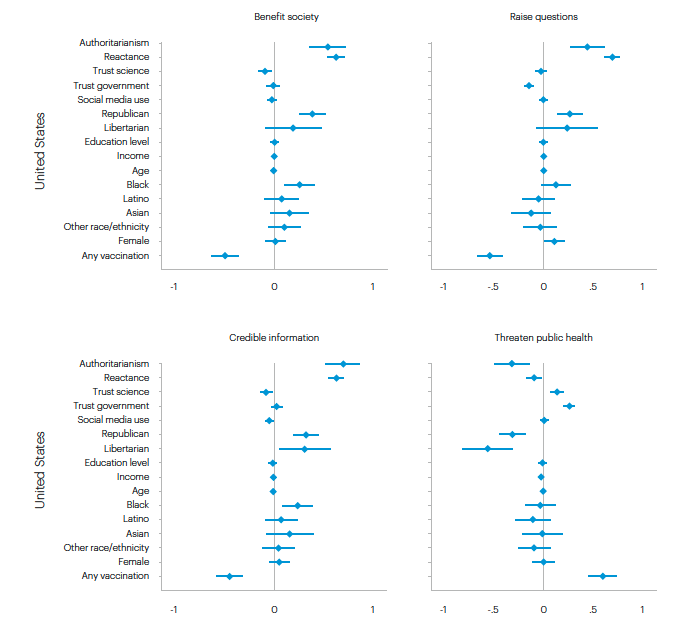
Figure 5: Correlates of attitudes toward anti-vaccination activism (UK respondents)
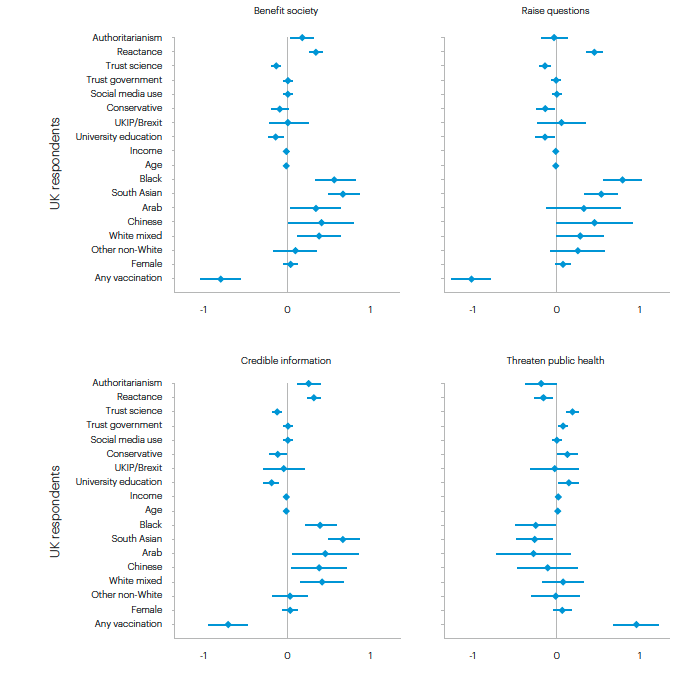
We summarise our findings as follows:
- Similar sets of factors to those that predict beliefs about vaccine safety/efficacy also predict respondent attitudes toward organised anti-vax activism, suggesting that countering anti-vaccine activism and the misinformation it disseminates may represent an important strategy for promoting vaccine uptake and minimising scepticism about vaccine safety and efficacy.
- In both the US and UK, respondents with more authoritarian attitudes and greater levels of psychological reactance are more likely to hold positive believes about anti-vax activist groups and less likely to view them as a threat, though the effect of authoritarian attitude is again weaker among UK respondents. In both samples, respondents with lower levels of trust in science are generally more supportive of anti-vax activism and less prone to view these groups as threats to public health.
- Political identity exerts a divergent influence in the US and the UK: in the US, Republicans are generally express more favourable opinions of anti-vaccine activist groups, while in the UK Tories express less favourable opinions of these groups.
- Black respondents in the US appear to be somewhat more supportive of anti- vax groups compared to other ethnic and racial groups. However, in the UK respondents from numerous minority groups (Black, South Asian, Arab, Chinese, and Mixed-race) are more positively inclined to anti-vax groups and their messages.
- Vaccination status is the most important predictor of attitudes toward anti-vax activism: unvaccinated respondents are, unsurprisingly, substantially more likely to express positive attitudes toward anti-vax activist organisations. Notably, however, the results summarised above hold even after account for vaccination status, suggesting that support for anti-vax messaging persists even among some segments that have received vaccinations.
Assessing and responding to anti-vax activist threats
As we discussed above, we anticipate that exposure to misinformation in the context of anti-vax protests increases COVID-19 vaccine hesitancy, increases belief in inaccurate information about COVID-19 vaccines, and promotes suspicion about authorities’ efforts to encourage vaccine uptake. Protest is a form of activism through which anti-vax groups disseminate information and promote their preferred narrative, which often involve (inaccurate) claims about the dangers of vaccines, their lack of efficacy, and the nefarious intentions of the authorities that produce and distribute them. Consequently, anti-vax protests promote vaccine hesitancy by explicitly cueing observers’ apprehensions and uncertainties about the trustworthiness of health and political authorities and by exploiting their limited knowledge of medical science.
Strategies of information dissemination should also influence how people respond to information. As we note above, current studies—and much of the government’s attention—have focused on the role of online activism is spreading myths and misinformation about COVID-19 and COVID-19 vaccines. Yet, there is reason to believe that conventional direct protest action should have a greater impact on observer beliefs. First, while social media memes and shared “news” stories are ubiquitous on social media, organised dissent is still rather rare. Observers are therefore likely to become increasingly desensitized to the effects of social media misinformation because the market for it has become saturated, thereby limiting the attention that the average observer devotes to it. By contrast, the relative rarity of protest actions—particularly those that draw substantial crowds or produce clashes with police or counter-protesters—render them comparatively novel, thus inviting more widespread attention and deeper interest. Consequently, we expect that exposure to misinformation via anti-vax protests will have a larger impact on observer attitudes about vaccine safety and efficacy than exposure to misinformation via social media.
We report the results of the first experiment in Figures 6 and 7. Figure 6 reports the regression results of models comparing the effect of the two forms of misinformation exposure (relative to the control) on subjects’ beliefs about the likelihood that vaccines harm specific groups.
Figure 6: Effects of misinformation on beliefs about group-specific harms
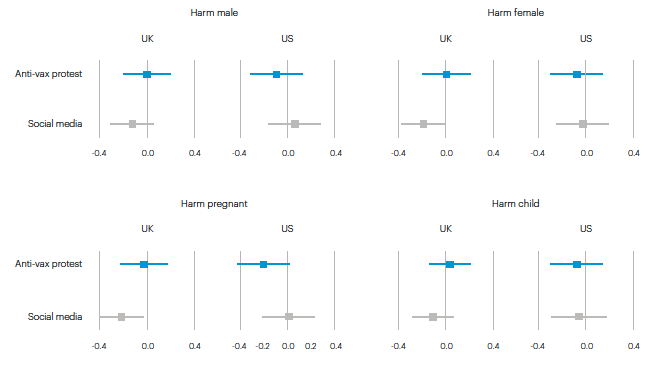
Figure 7: Effects of misinformation on beliefs about side effects
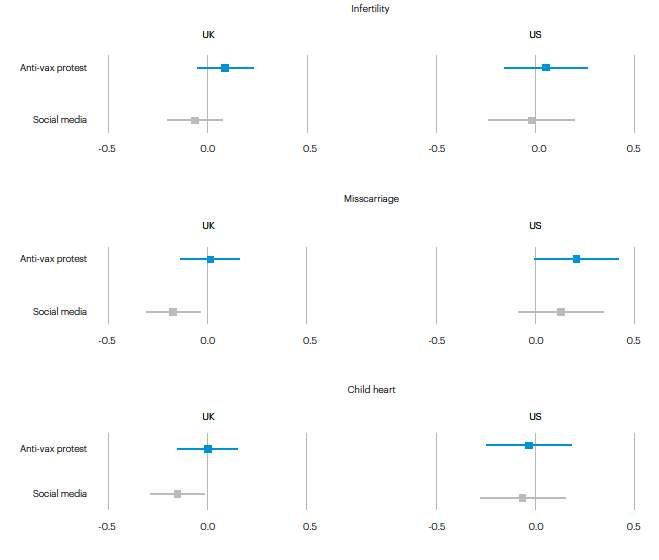
Based on these results, we conclude the following:
- Exposure to misinformation regarding the potential harms associated with COVID-19 vaccines does not increase respondent scepticism about the safety of the vaccines.
- Respondents exposed to a news article that described a hypothetical anti-vaccine protest and included specific claims about the harms associated with COVID-19 vaccines (e.g., infertility, miscarriages, etc.) and the risk of harms to specific groups (e.g., women and children) were no more likely than those exposed to a treatment article (ant-climate protest story) to believe that vaccines harm specific groups or cause specific serious side effects.
- Respondents exposed to a fabricated social media post by a hypothetical anti-vax group and including the same misinformation were (surprisingly) somewhat less likely to believe that vaccines harm specific groups or cause specific serious side effects.
The manner in which political and health authorities respond to misinformation should also moderate the influence of protest exposure on vaccine hesitancy. We expect that interventions by apolitical authorities (such as individual GPs/family doctors) may effectively counteract the adverse influence of misinformation exposure on vaccine hesitancy. By contrast, efforts by political authorities, such as elected representatives or government officials, will be largely ineffective at countering misinformation. Moreover, we anticipate that overt condemnation and criticism of the protesters will have limited ability to counteract misinformation and may, in some cases, result in backlash.
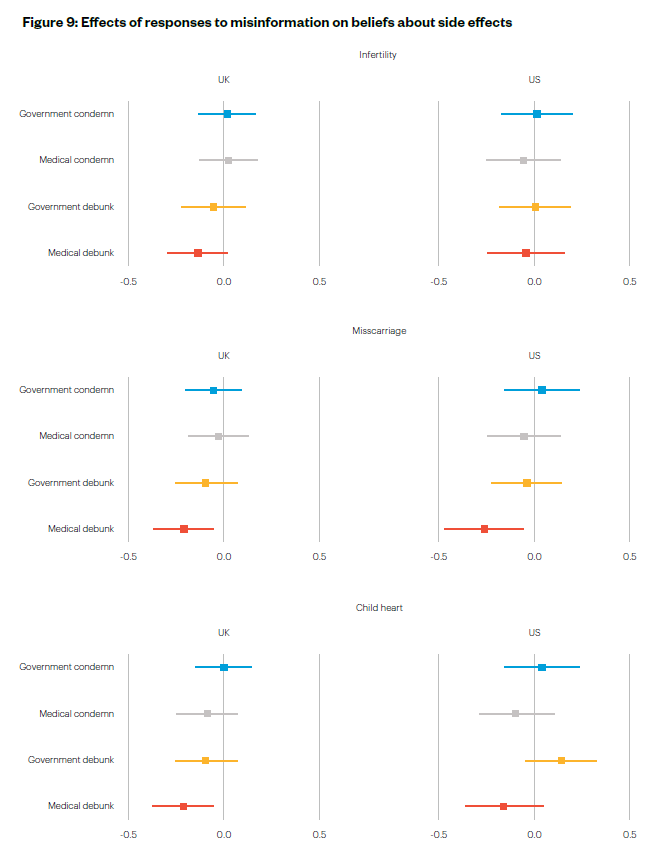
Figures 8 and 9 show the effects of different forms of responses to misinformation by government authorities and medical professionals on respondents’ attitudes toward the risks and harms association with COVID-19 vaccines. Figure 8 shows the effect of the treatments on respondents’ beliefs about the potential for COVID-19 vaccines to harm specific groups, while Figure 9 shows the effect of the treatment conditions on beliefs about specific severe side effects. As before, each plot within each figure includes results for the UK (left) and US samples.
In brief, our results suggest the following:
- Debunking misinformation is an effective strategy for counter inaccurate beliefs about the risk of harms associated with vaccines—if it comes from health professional.
- Respondents that were exposed to a news story that included statements delivered by healthcare professionals (GPs, physicians, etc.) that explicitly countered or corrected anti-vaccine misinformation were generally less likely to believe that vaccines harm specific groups or cause specific serious side effects. This effect was strongest in the sample of UK respondents.
- Debunking statements by political authorities (MPs, congress persons, etc.) were ineffective at countering misinformation. Statements of condemnation by either type of authority had no effect on respondent beliefs about vaccine harms.
Figure 8: Effects of responses to misinformation on beliefs about group-specific harms
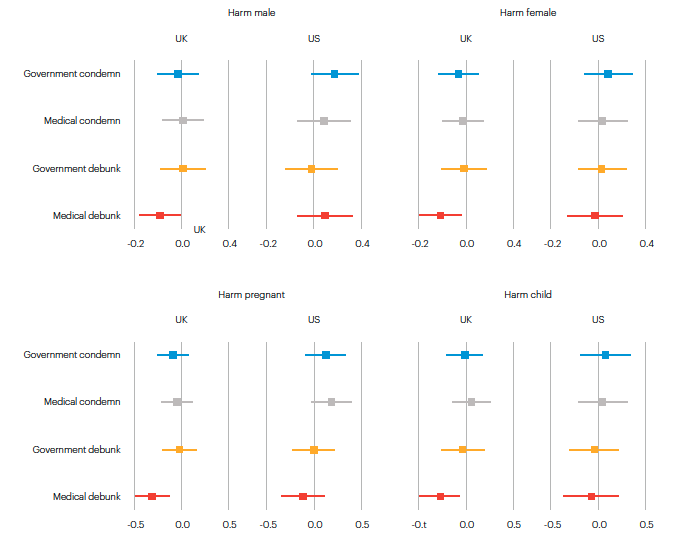
Figure 9: Effects of responses to misinformation on beliefs about side effects
Discussion and implications
Through the studies presented in this report, we have sought to extend the understanding of vaccine hesitancy in a few key ways. First, our findings highlight the centrality of perceptions of vaccine efficacy and safety to an individual’s intent to vaccinate. While the relationship seems obvious, most existing studies have focused principally on whether or not an individual intends to vaccinate or has previously received a vaccination. Yet, it is likely that apprehensions about the specific potential risks associated with vaccines rather than diffuse fears about vaccine safety, the perceived cost-benefit balance between disease risk and vaccine risk, and specific beliefs about the efficacy of vaccines influence uptake. The results of our multi-wave survey, which was deployed to a large, representative samples of respondents in the US and the UK, provides strong evidence for this claim. Safety and efficacy concerns are among the primary explanatory factors in our models of vaccine status, including booster status. Once we account for these attitudes, several of the predictors identified in earlier studies become insignificant.
This finding highlights the importance of directly addressing individuals’ fears about vaccine risks and improving knowledge about the efficacy of the vaccines in preventing serious illness from COVID-19. Concerted efforts to counter these fears will likely be an important aspect of efforts to reduce vaccine hesitancy and promote uptake in reluctant or ambivalent communities. The results from the experiment that we embedded in our broader survey provide some evidence of the potential effectiveness of these strategies. In the UK wing of our study, we found consistent evidence that respondents’ beliefs about harms associated with COVID-19 vaccine diminished when members of the medical community corrected misinformation about the risks of the vaccines. Such debunking was particularly effective at reducing concerns that vaccines harmed women, pregnant women, and children and that they caused miscarriages and damaged children’s hearts. Such claims are commonly made by anti-vaccine activists, and have likely discouraged many individuals from accepting vaccines. Encouragingly, however, exposure to corrective messages from health professionals may be able to ameliorate those fears and reduce vaccine hesitancy, at least among the population of the United Kingdom. It is important to underscore that, however, that the effect is only observed when corrections are made by medical professionals such as doctors/physicians. Corrections by government and political authorities had no discernible influence on respondents’ beliefs about the safety of COVID-19 vaccines. Thus, the messenger matters in terms of efforts to correct misinformation.
Our analyses also shed new light on public attitudes toward organised anti- vaccination groups, as well as the effects of misinformation disseminated by these groups. Misinformation plays an important role in the promotion and perpetuation of vaccine hesitancy. Much of this information developed and spread by organised groups of anti-vaccine activists. The abrupt and unexpected arrival of the novel SARS-CoV-2 virus and the scramble to understand and manage it created significant opportunities for extant anti-vaccine groups to mobilise and disseminate their beliefs. While still often regarded as “fringe”, the number of such groups has multiplied during the course of the pandemic. They have also become increasingly vocal and increasingly militant. Their activities include not only the dissemination of misinformation via social media, but also public marches and protests, protests targeting schools and school children, harassing journalist, government officials, teachers, and health workers, military style training activities, and confrontations with police.(9) Through our survey, we therefore sought to understand what factors influence individuals’ attitudes toward such groups and what effect exposure to the group’s activities has on attitudes towards vaccines.
Analyses of our survey data suggest that similar factors predict respondents’ beliefs in inaccurate information about the potential harms of COVID-19 vaccines as well as their attitudes toward organised anti-vaccination activism. For example, in both samples, individuals with higher scores on the scales of psychological reactance and authoritarian attitude are more likely to believe that such groups benefit society and share credible information about COVID-19 and vaccines and are less likely to view them as a threat to public health. This is particularly true in the US sample. Similarly, race/ethnicity as well as political identity influence these attitudes. In the US, Black individuals are more likely than other ethnic or racial groups to view the groups as beneficial to society and believe in the credibility of their information. In the UK, membership in one of several different non-White groups is associated with a greater likelihood of such beliefs.
Identifying the factors that shape an individual’s beliefs about anti-vax movements may also help predict which groups or individuals are most susceptible to the myths and misinformation that such groups promulgate. For example, the empirical observation that members of minority groups are more likely to see organised anti- vax groups as benign or beneficial might imply greater vulnerability to anti-vax misinformation—or possibly the success of anti-vax groups in shaping attitudes within those communities. This observation might provide opportunities for targeted efforts to counteract the influence of anti-vax misinformation, thus reducing vaccine hesitancy within that community.
The results of our experiment offer encouraging yet tentative evidence that such intervention might prove effective at combating misinformation and promoting confidence in COVID-19 vaccines. We find that when health professionals directly correct or debunk anti-vaccine misinformation, respondents’ beliefs that vaccines cause harms to specific groups and cause serious side effects decline. By first identifying populations and communities that are inclined to view anti-vaccine activism as beneficial and their messages credible, public health strategists could more efficiently direct resources intended to challenge and counteract the misinformation disseminated by these groups.
References
Branton, Regine, Valerie Martinez-Ebers, Tony Carey, Jr. and Tetsuya Matsubayashi. 2015. “Social Protest and Policy Attitudes: The Case of the 2006 Immigrant Rallies”, American Journal of Political Science 59(2): 390-402.
Burki, Talha. 2019. “Vaccine Misinformation and Social Media”, Lancet Digital Health 1 (6): 258-259. Challenger, Aimée, Petroc Sumner and Lewis Bott. 2022. “COVID-19 Myth-busting: An Experimental Study”, BMC Public Health 22 (131).
Cornwall, Warren. 2020. “Official Gird for War on Vaccine Misinformation”, Science 369: 6499
Loomba, Sahil, Alexandre de Figueiredo, Simon Piatek, Kristen de Graaf and Heidi Larson. 2021. “Measuring the Impact of COVID-19 Vaccine Misinformation on Vaccination Intent in the UK and USA”, Nature Human Behaviour 5: 337-348.
Neely, Stephen, Christina Eldredge, Robin Ersing and Christa Remington. 2022. “Vaccine Hesitancy and Exposure to Misinformation: A Survey Analysis”, Journal of General Internal Medicine 37: 179-187.
Pierri, Francesco, Brea Perry, Matthew DeVerna, Kai-Cheng Yang, Alessandro Flammini, Filippo Menczer and John Bryden. 2021. “The Impact of Online Misinformation on US COVID-19 Vaccinations”. Pre-print. https://arxiv. org/ftp/arxiv/papers/2104/2104.10635.pdf
Roozenbeek, Jon and Sander van der Linden. 2022. “How to Combat Health Misinformation: A Psychological Approach”, American Journal of Health Promotion 36(2)
Wouters, Ruud. 2019. “The Persuasive Power of Protest: How Protest Wins Public Support”, Social Forces 98(1): 403-426.
Appendix 2
Figure A1: COVID-19 vaccination rates
Figure A2: Beliefs about COVID-19 vaccines
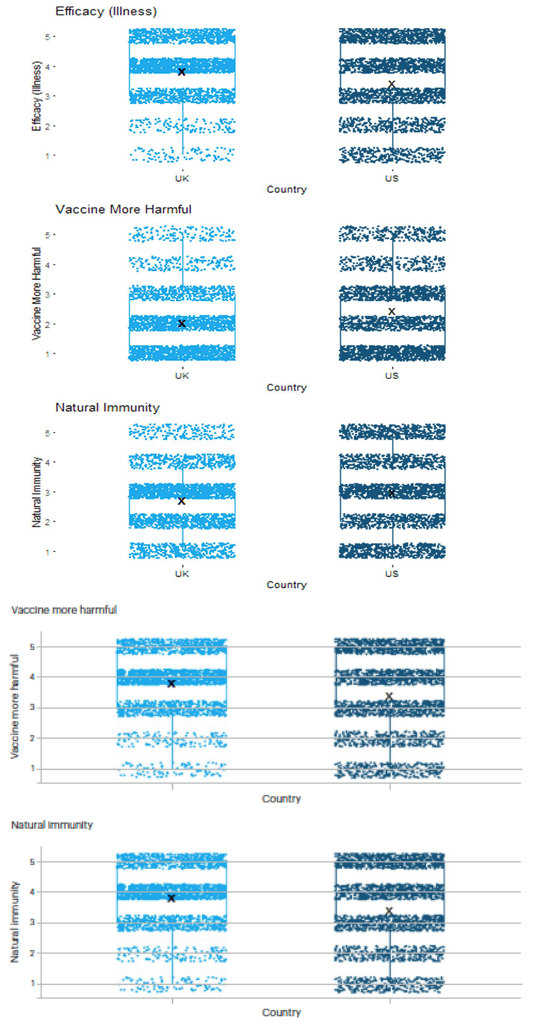
Figure A3: Belief in group-specific harms from COVID-19 vaccination
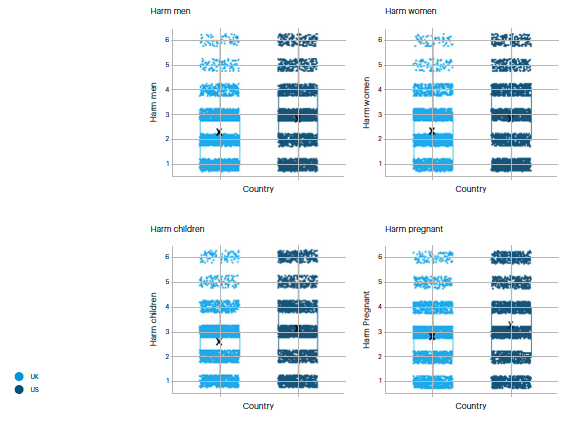
Figure A4: Belief in side effects from COVID-19 vaccination
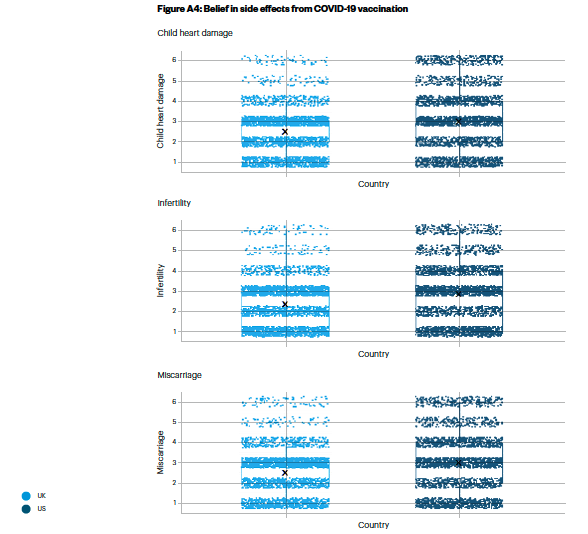
Figure A5: Attitudes toward anti-vaccination activism
Citations
- Wave 1 was fielded between 17 January 2022 and 21 January 2202, while Wave 2 was deployed between 7 February 2022 and 16 February 2022.
- Summary statistics and descriptions of key variables used in the analyses are included in Appendix 1. We present additional descriptive statistics for UK and US vaccine status and beliefs in Appendix 2.
- Theories of psychological reactance posit that when individuals perceive a loss of freedom and autonomy, they will experience a sense of anger and negative feelings (“reactance”), which in turn motivates them to attempt to re-establish that freedom. Authoritarian attitudes reflect respect for traditional social hierarchies, obedience to authority, and support for traditional power structures.
- Rozenbeek et al. 2020
- Burki 2019; Cornwall 2020
- Loomba et al. 2021
- Nealy et al. 2022
- See, for example, https://news.sky.com/story/covid-19-four-police-officers-injured-after-violence-breaks-out-at-anti-vaccine-protest-in- london-12398467; https://www.bbc.co.uk/news/59870550; https://www.economist.com/asia/2021/11/27/antipodean-anti-vaxxers-are- learning-from-americas-far-right
- See, for example, https://www.bbc.co.uk/news/59870550; https://www.independent.co.uk/news/uk/home-news/antivaccine-antivaxx- mhra-protest-london-b1913877.html; https://www.nytimes.com/2021/09/03/world/canada/vaccine-passports-protests.html; https:// www.theguardian.com/world/2021/oct/25/keir-starmer-schools-protected-anti-vaccine-protests-labour-exclusion-orders-priti-patel; https://www.bbc.co.uk/news/uk-england-london-58440700; https://abcnews.go.com/US/police-arrive-canada-us-border-disperse- truck-protesters/story?id=82845259
Summary
- Published
© The authors. This is an open access publication licensed under a Creative Commons Attribution-NonCommercial- NoDerivs 4.0 Unported License
To cite this report: British Academy (2022), Mobilised Misinforamtion: Addressing COVID-19 vaccine hesitancy and responding to anti-vax activism, The British Academy, London
- DOI doi.org/10.5871/c19-recovery/M-J-M-R-S-Z (Opens in a new window)