“Medicine is Still Against Black People”
Mapping and visualising intersections of social inequalities, community mistrust, and vaccine hesitancy in online and physical spaces in the UK and US
By Ozge Ozduzen, Billur Aslan Ozgul, Bogdan Ianosev, Alireza Karduni, Nelli Ferenczi, Wenwen Dou, Matthew Adams and Monika Frątczak
Download PDF report
- Published by
- British Academy
- Year
- 2022
- Pages
- 31
About the authors
Dr Ozge Ozduzen is a lecturer in Digital Media and Society at the University of Sheffield. Dr Billur Aslan Ozgul is a lecturer in Political Communication in the School of Social and Political Sciences at Brunel University London. Bogdan Ianoșev is a PhD candidate at the Glasgow School for Business and Society at Glasgow Caledonian University and Research Assistant at the University of Sheffield. Dr Alireza Karduni is a Postdoctoral Scholar Jointly at Northwestern University’s departments of Computer Science and Psychology. Dr Nelli Ferenczi is a lecturer in Psychology and a member of the Centre for Culture and Evolution at Brunel University London. Dr Wenwen Dou is an associate professor in the College of Computing and Informatics and a core faculty member at Charlotte Visualization Center at the University of North Carolina at Charlotte. Matthew Adams is a doctoral researcher in the division of Anthropology and a research assistant at the Brunel University College of Business, Arts, and Social Science. Dr Monika Fratczak is a researcher at the Department of Sociological Studies at the University of Sheffield.
About the COVID-19 Recovery: Building Future Pandemic Preparedness and Understanding Citizen Engagement in the USA and UK Series
The programme is the result of a partnership between the British Academy, the Social Sciences Research Council (SSRC) and the Science & Innovation Network in the USA (SIN USA) to award funding to ten transatlantic studies focusing on UK-US COVID-19 vaccine engagement. It follows a pilot study exploring levels of vaccine engagement in four locations across the US and UK, while the larger programme was expanded to study multiple locations. The programme was funded by the UK’s Department for Business, Energy and Industrial Strategy.
Executive summary
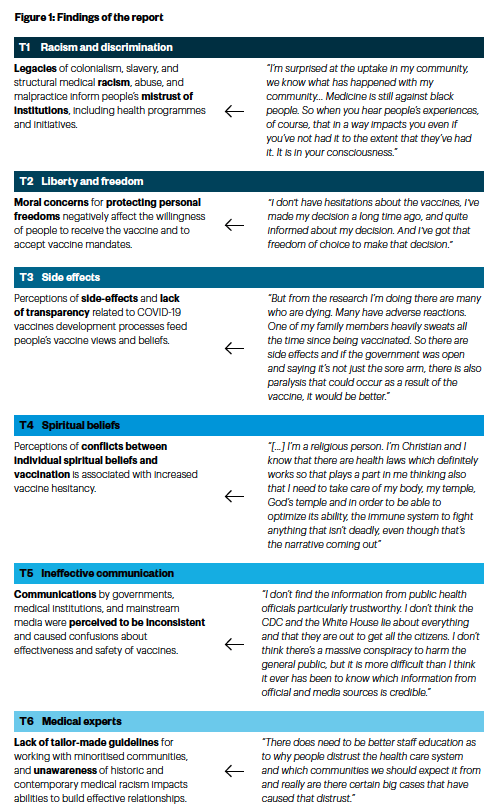
Funded by the British Academy, this report is part of a research project entitled “Mapping and visualising intersections of social inequalities, community mistrust, and vaccine hesitancy in online and physical spaces in the UK and US”. The report investigates social, cultural, and political factors underlying vaccine hesitant beliefs and ideas among minoritised communities in the United Kingdom (UK) and the United States of America (US). The data is collected through interviews and focus groups with vaccine-hesitant individuals within various religiously, ethnically, and racially minoritised communities, interviews with medical practitioners, and through thematic analysis of vaccine communication in Twitter and Telegram during the COVID-19 pandemic. Based on our findings (see Figure I), we suggest five strategic goals for policymakers to pursue:
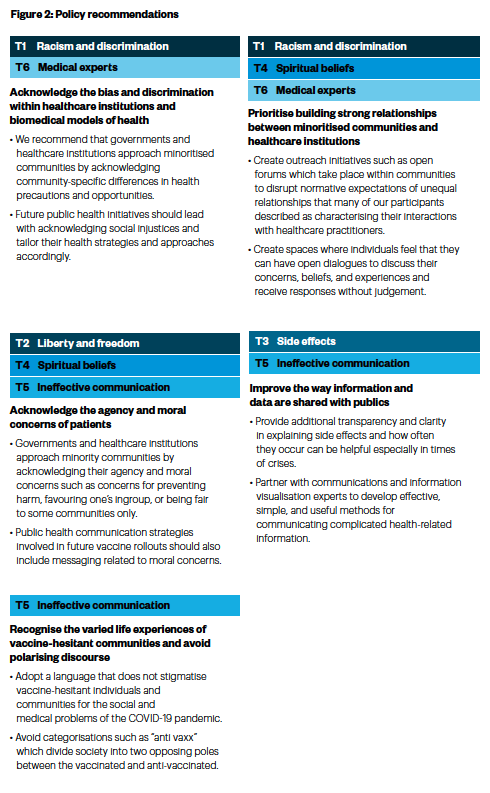
Acknowledge the bias and discrimination within healthcare institutions and biomedical models of health: Instead of a one size fits all approach, policies and decisions must be made by acknowledging social injustices as well as the historic and ongoing medical mistreatment of minoritised communities. Any possible side effects of the COVID-19 vaccine on minoritised communities need to be investigated and shared with the public. Official messages should also acknowledge past and ongoing injustices and racism and assure the public that every precaution is taken to avoid any repetition of the past. Importantly, equipping medical practitioners with knowledge of systemic medical racism and minoritised communities’ lived experiences through formal training will contribute to building trust.
Prioritise building strong relationships between minoritised communities and healthcare institutions: To build trust and disrupt unequal relationships that many of our participants described as characterising their interactions with healthcare practitioners, we propose outreach initiatives such as open forums which take place within communities. Where possible, these community outreach projects should include trusted members of communities, including religious leaders, and medical experts.
Acknowledge the agency and moral concerns of patients: Governments and healthcare institutions in the US and UK should consider approaching minoritised communities by acknowledging their agency and moral concerns around the COVID-19 vaccine such as concerns for perceived harm of vaccine, favouring one’s ingroup, or being fair to some communities only.
Improve the way information and data are shared with publics: We suggest that in future communications, additional transparency, and clarity in explaining side effects and how often they occur can be helpful for governments and healthcare institutions during challenging historical moments, such as the COVID-19 pandemic. For communicating complicated health-related information, governments and policymakers should partner with communications and information visualisation experts to develop effective, simple, and useful resources and materials.
Recognise the varied life experiences of vaccine-hesitant communities and avoid polarising discourse: public institutions including media companies need to adopt language that does not stigmatise vaccine-hesitant individuals and communities for the social and medical problems of the COVID-19 pandemic. Stigmatisation leads to fear of social punishment or financial costs such as losing employment and prevents the vaccine hesitant public from expressing themselves and their needs. News articles which generalise vaccine-hesitant people and call them “anti-vaxx” might also prevent the public from understanding the different experiences and reservations of vaccine hesitant communities.
Figure 1: Findings of the report
Introduction
The COVID-19 pandemic has exacerbated existing social inequalities, impacting those who are most vulnerable and putting racial and ethnic minority communities more at risk of getting sick and dying.(1) The vaccine rollout has been touted as key to providing a firebreak in infections at the community level. However, sizable disparities in vaccination uptake between the majority and minoritised populations have emerged both in the US and the UK. According to the UK Office for National Statistics Public Health Data Asset (by 31 December 2021), white British (68.4%), Indian (65.3%), and Chinese (64%) groups were more likely to receive three vaccinations than Black Caribbean (33.9%), Pakistani (37.8%), and Black African (37.9%) ethnic groups in the UK.(2) The proportion is also lower among Muslims in comparison to other religions. In the US, COVID-19 vaccine mistrust is widespread among Black Americans and Hispanics,(3) while Black Americans are more hesitant about receiving the COVID-19 vaccine relative to other American populations.(4)
So far, there is a lack of evidence-based interventions to reduce vaccine hesitancy.(5) Our recommendations for bridging historic divisions between minoritised communities and healthcare institutions centre around building space for open conversation between medical practitioners and minoritised communities about their concerns regarding the COVID-19 vaccine, which acknowledges legitimate distrust and historical and contemporary structural medical racism. Furthermore, by highlighting the multifaceted experiences of vaccine-hesitant communities, this report seeks to further dispel some of the embedded prejudices surrounding these group identities. Our approach has uncovered several ways in which more or less universal themes in reasoning interact with intersectional social identities, experiences of historical and contemporary discrimination, moral preferences, and personal differences which collectively give rise to vaccine hesitancy.
We thus aim to address multiple research questions in this report. First, we ask whether experiences of historical oppression have informed attitudes and decisions of minoritised communities towards public health mandates and vaccines. Second, we explore contemporary mistreatment and discrimination of minoritised communities in the UK and US and how this affects the trust towards public health initiatives, such as vaccination programmes. Third, our report uncovers whether there are other factors that fed into vaccine hesitancy during the COVID-19 pandemic, such as religious beliefs and exposure to mainstream media. Fourth, we address the ways in which social media is used among vaccine-hesitant communities and explore how the interaction of vaccine-hesitant communities inform vaccine-hesitant views, beliefs, and protest organisation. Finally, instead of assuming that vaccine hesitancy is mainly caused by patient attitudes and beliefs, we adopt a ‘symmetrical’ research design and analyse if there are systemic prejudices of medical communities and the way that these prejudices reproduce and reinforce vaccine hesitancy among minoritised communities.
To answer these questions, the report uses three different but interrelated sets of data to capture online and offline discourses related to the COVID-19 vaccine. The report is, first, based on interviews and focus groups with racially, ethnically, and religiously minoritised communities in the US and UK, conducted in January, February, and March 2022 during the COVID-19 pandemic. As social relationships and shared communities form one of the backbones of this research, we primarily used a snowball approach in our recruitment by asking participants in our interviews if they would be willing to share our study with their social network. We also recruited research participants by using social media advertising through our personal social networks, the institutional social media profiles of our universities, and by posting our Google Forms on vaccine-hesitant and anti-vaccination channels and groups on social media platforms. Furthermore, we used the Participant pool on Prolific Academic to recruit some of our participants.
In our recruitment, we informed participants that two of the inclusion criteria adopted in this study were: 1) they self-identify as vaccine-hesitant and 2) as a member of a religiously, racially, or ethnically minoritised community. This was included in our recruitment adverts and the participant information sheet. This addresses the issues of researchers (often in positions of power) from ascribing and judging who is a minority. To understand the (il)logic of social stratification, cultural marginalisation, or inequality, we need to appreciate the deep and complex interpenetration of race, class, gender, and sexuality. Race, however, has played a unique role in the formation and historical development of the United States and United Kingdom.(6) Coming to an understanding of the structural embeddedness of racism in Western societies, including medical racism, necessitates a historical perspective that shows how the universalising rationalisation of human differences effectively shaped the acceptability of exclusion.(7) Minorityhood thus refers to the degree of social power and for there to be minorities there needs to be a majority that holds more social power.(8) In this context, minority as a term refers to groups that are subjected to oppression, discrimination and exclusion by the majority, in other words, those in more powerful social positions.(9) Because of the ways that shared cultural norms and expectations function, and members of dominant groups are privileged, it is members of minoritised communities themselves who will know that they are marginalised/minoritised by the dominant groups. These identities are intersectional, with our research participants reporting racial, ethnic, cultural (e.g., nationality), and religious identities which are minoritised– and at times reporting several minoritised identities. Having said this, the largest minoritised community in both the US and UK was Black (African American, Black British, Black Caribbean and Black immigrant) research participants, followed by mixed race participants for both contexts, Hispanic for the US and South Asian for the UK.
We also drew on two population samples for our interviews: 1) ethnically, racially, and religiously minoritised communities that are vaccine-hesitant; 2) minoritised communities who joined the anti-vaccine passport protests. This granted us a deeper understanding of protesters’ own voice in choosing not to participate in the COVID-19 vaccination programme and rather selecting to protest against perceived vaccine mandates. In total, we conducted 27 interviews in the UK and 13 interviews in the US with vaccine-hesitant people among minoritised communities. In addition to interviews, we held two focus groups with vaccine-hesitant groups in the UK (with four participants) and US (with five participants) which provided the report with a nuanced understanding of discourses around specific social and historical problems, concerns, reservations, and issues that minoritised communities raised about the COVID-19 vaccines. In order to understand the doctors, nurses and other healthcare professionals’ engagement with vaccine-hesitant patients in the COVID-19 pandemic, we held eight interviews with medical practitioners in the UK and six interviews with medical practitioners in the US. Overall, we conducted 54 in-depth interviews and two focus groups in the US and UK.
Finally, in the process of our interviews and focus groups with minoritised communities, we identified Twitter and Telegram as important news sources for many in vaccine-hesitant communities. To explore and analyse the social media conversations of anti-vaccine and vaccine-hesitant communities, the report is thus based on medium size social media data collection and analysis, harnessed from Telegram and Twitter. Twitter is a public-based social media platform, which allows for the dissemination of ‘bitesize’ information. For Twitter, we used hashtags and mentions at the intersection of racial discourse and COVID-19 vaccines. Our Twitter dataset included keywords, namely #BLM, #BlackLivesMatter, and #vaccine, and was composed of more than 70,000 tweets (including duplicate retweets) and 19,211 unique tweets (excluding retweets).
Telegram is primarily a messaging app that provides private and group messaging functionalities. Since Telegram generally does not enforce regulations around misinformation, messages that are usually removed and banned on Twitter and other platforms are observable on Telegram. The hybrid nature of Telegram (e.g., private chat, public chat, and channels) has made it a popular platform for collective action such as the organisation of protests and sharing of information in more covert ways.(10) We identified popular Telegram channels focused on general COVID-19 information (e.g., protests, organisation, news circulation) and ones that are focused on vaccine side effects. The first account, Covid Red Pills, a US-based channel, yielded 8,105 total messages; the second account, TRUTH PILLS, a UK-based channel, yielded 4,819 total messages. In order to understand the side effects and injuries Telegram users are concerned about, we also collected messages from the Covid Vaccine Injuries Telegram channel that contained 10,646 messages. Messages from these three accounts were combined, cleaned, and processed and we employed a mixed-method approach to analyse Telegram and Twitter text data. First, we summarised a large corpus of text using topic modelling. We then qualitatively evaluated and thematically analysed the most prevalent automatically extracted topics within our datasets.
Using these datasets, this report shows that our ethnically, racially and religiously minoritised vaccine-hesitant participants’ reasoning, motivations and decision-making were informed by a host of salient factors including 1) cost-benefit evaluations related to vaccine side-effects, 2) mistrust towards institutions and official health messaging 3) sensitivity towards past and contemporary social injustices and discrimination, 4) engagement and interaction with social and legacy media, 5) religious and spiritual beliefs as well as 6) moral concerns such as personal freedom and concerns about social costs. However, our findings also indicate that not every participant is affected by all these factors. Each community has distinctive characteristics and backgrounds (e.g., their religion, immigration status, ethnic identity) and these feed into their vaccine beliefs.
The report consists of two main sections, namely our findings and policy implications and recommendations. The report first uncovers vaccine hesitancy themes in minoritised communities through an analysis of interviews, focus groups and social media conversations on the COVID-19 vaccine during the pandemic. The ensuing section explores the unquestioned structural biases of medical practitioners and the challenges they face in their interactions with vaccine-hesitant patients during the pandemic. The final part of the report provides five strategic policy suggestions as a useful starting point for policy engagement and change on vaccine hesitancy, social inequalities, and community mistrust.
Findings
T1. Racism and discrimination: Historical legacies and contemporary discrimination affect vaccine hesitancy
Minoritised communities in the US and UK have experienced a troubled history of neglect, racism, and discrimination by healthcare institutions who were either unwilling or unable to cater to their needs,(11) (12) (13) (14) the impact of which is still readily observed, as evidenced in our interviews and focus groups. The evidence clearly shows that histories of abuse, neglect, discrimination and racism left lasting marks on the health decisions of ethnically, racially, and religiously minoritised communities in the US and UK today. Our interviewees referred to historical legacies of colonialism, slavery, and historical malpractice, engendering mistrust of institutions vividly. As known instances of historical discrimination and abuse, they particularly mentioned the Tuskegee Syphilis Study and the story of Henrietta Lacks, which led our research participants to cautiously engage with the present healthcare programmes and mandates. An important difference between our interviews and focus groups in the UK and the US is that, our participants’ accounts of historical discrimination were immediate and embedded in participants’ very thought processes in the US. On the other hand, Black communities in the UK recounted such events with an implicit distance and took more time to recall, a sign of a difference in the degree and scope of discrimination on our participants’ lived experiences between the two nations.
Our Black participants perceived research on medicine to be racist and geared towards White people’s bodies and needs. Our informants thus pointed out their concerns and reservations towards the COVID-19 vaccine’s perceived side effects to different body compositions and perceived threat of potential trials to be conducted on their own communities. Our Black participants also reported not having received the attention that they expect from the medical professionals. Our Black research participants also highlighted that their physical pains have been institutionally minimalised by White medicine and medical professionals. During our fieldwork, ethnic and racial minorities in the US also reported lower quality health care, and their perception that hospitals primarily dedicated to Black and Hispanic patients were underfunded. Likewise, the evidence shows that racial discrimination is a key contributor to healthcare inequalities in the UK. The unsatisfactory treatment of some of these communities in both the UK and US fuels mistrust of the healthcare system, including the vaccines recommended by the same system.
Our research participants who are part of other racially, ethnically, or religiously minoritised communities (e.g., second generation Hispanics, Middle Easterners, Eastern Europeans, Muslims), also often referred to their own or their parents’ and grandparents’ lived experiences of overt discrimination and blatant racism within healthcare institutions in the UK and US. These experiences ranged from discriminatory and racist remarks to sexual innuendos. In some instances, participants also reported discrimination due to their accents in English. Language barriers were highlighted to lead to a lack of interest from medical doctors in patients’ symptoms and problems. This informed their mistrust of healthcare practitioners and systems, including their understanding of and reaction to the COVID-19 vaccine.
Moreover, we found out that past and contemporary medical malpractice on Black people affected health decisions of African Americans much more directly, including their engagement with the COVID-19 vaccine. Participants from the US experienced instances of shattered trust in medical practitioners as a result of neglect experienced at previous medical visits, which impacts on their vaccine beliefs and decisions today. Our research participants also shared experiences and perceptions of not belonging to the healthcare system due to their ethnic and racial identities, feeling discomfort while being treated, experiencing neglect and belittlement, feeling judged by medical professionals for being vaccine-hesitant, experiencing poor care with many instances of misdiagnoses and poor communication with medical practitioners.
Our findings indicate that these experiences motivated minoritised communities, who currently self-identify as vaccine-hesitant or anti-vaccine, to search for alternative health solutions, including first or second-generation immigrants having to travel to their countries of origin to receive healthcare if they were first or second-generation immigrants. Experiencing discrimination and marginalisation also led minoritised communities to seek medical practitioners from their own ethnic, racial, or religious communities and some of our research participants claimed seeking healthcare professionals who share their values and experiences. This exemplifies a perceived lack of shared knowledge between minority patients and White healthcare providers. Some of our research participants reported experiencing ingroup marginalisation as well as society-wide marginalisation and alienation due to their vaccine beliefs.
We have also found that there were no community-specific guidelines for medical practitioners when serving patients from different communities during the COVID-19 pandemic. Instead, public health initiatives in the UK and US seemed to have been informed by a ‘one-size-fits-all’ approach, which assumes a homogenous target audience. It also appears that this approach is designed under a mostly majority White, possibly middle class, outlook since it fails to take into account pervasive differences in life opportunities available to individuals from different communities.
T2. Liberty and freedom: Concerns for infringements of individuals’ liberty and freedom affect vaccine hesitancy
One of the foremost themes from our research is that of moral concerns for individual freedoms and the perception that the vaccine mandates restrict individual freedoms. Our vaccine-hesitant and anti-vaccine research participants believe that vaccine mandates represent a moral issue and that nobody should force anyone to get a vaccine if they do not want to. Our UK research participants explicitly identified themselves as ‘pro-choice’ in the vaccine debate. However, the majority of our US participants chose not to self-identify as pro-choice even though they were aware of this identifier and the encompassing debate. The concerns for personal freedoms were rather associated with negative views towards any kind of government-issued mandates, but especially towards both vaccine passports and vaccine mandates. Participants either explicitly referred to mandates and passports as morally wrong, or else mentioned the importance of protecting one’s freedoms of choice regarding personal or medical matters in association with other reasons why vaccine mandates are wrong. Among these reasons, there were doubts about the scientific development of the COVID-19 vaccines, reactions to societal control mechanisms, fears of tyrannical state policies, religious beliefs, mistrust of governments and pharmaceutical corporations, libertarian beliefs, and conspiracy theories. For instance, one of the participants identified the vaccine passports as a monitoring tool, where what you do and where you do it is monitored.
Our findings show that our research participants’ mistrust of government and public health initiatives were also directly linked to the perceived lack of a genuine public debate surrounding vaccines and vaccine mandates. Instead, our participants reported that they experienced social pressure towards getting vaccinated. Some of them even indicated that they were harassed to get the COVID-19 vaccine. As a result of the moral debate over vaccination, participants observed that vaccine beliefs tend to make the society politically polarised. Due to this polarisation, our findings reveal that vaccine-hesitant research participants perceived certain social costs for advertising their vaccine beliefs in social groups who may not agree with them. To this end, one participant recounted that they kept their vaccine beliefs to themselves as a precaution and so as not to risk losing their job. Other research participants also steered clear of vaccine debates after their experience of being blamed and stigmatised for their beliefs, feeling marginalised, or being labelled as conspiracy theorists.
Our research participants also did not trust government health initiatives as they perceived that such initiatives convey inconsistent information, for instance, contradictory advice regarding mask use and vaccine efficacy. Some of the participants also mentioned that official scientific information tended to change as newer data was periodically analysed and this reduced their trust towards official scientific advice. Likewise, the additional requirement for the COVID-19 booster shots was perceived by our participants as a sign that the trials were not over before the vaccine roll-out commenced. As one participant highlighted, first the government proposed a vaccine to end the pandemic, then a second dose was also required, then a booster, and so on. Public health officials may have expected most of the public to be aware of the fact that numerous other vaccines also require several doses. However, our interviews revealed that the appearance of boosters is rather considered as a failure of previous scientific information and data by vaccine-hesitant minority communities.
A few participants also mentioned that the UK government’s initial plan to go with a herd immunity approach,(15) only for it to be scrapped shortly thereafter, bolstered further mistrust of the government’s health advice. Hence perceived conflicting government narratives further fuelled the vaccine hesitancy of our interviewees. Additionally, the breaching of social distancing measures by government members during the pandemic exacerbated further mistrust towards the lockdown measures and vaccination programmes proposed by the same people. In the US, some participants confessed a tentative willingness to engage more with government advice if the government admitted that it was unsure about what measures would best to mitigate the impact of the pandemic. Our participants were concerned that the US government was instead pressuring its citizens to accept ready-made health decisions on their behalf.
Perceived inconsistency of pandemic policies coupled with perceived disappointments of medical science further erode trust among our participants, some of whom discussed the absence of any logic in government initiatives. When citizens feel constrained and obligated to undertake physically intrusive procedures such as receiving vaccines, while simultaneously feeling that their moral concerns are not listened to, they are likely to become cautious and suspicious about the COVID-19 vaccine. This plays into the multitude of other reasons driving vaccine hesitancy. Because moral concerns are fundamental to human life, vaccine mandates can appear as an encroachment on fundamental moral rights to citizens who think these mandates threaten their liberty and freedom. When patients already feel that their concerns are not being listened to, avoiding patients’ agency and core concerns in designing public health policy can seem rather paternalistic. These grievances can be read as a backlash to paternalistic pandemic policies where individuals are not viewed as moral, rational, and active agents but rather as passive targets for public health policy.
T3. Side effects: Side effects and health hazards affect vaccine hesitancy
The findings of our research also reveal that perceived side-effects and health hazards of the COVID-19 vaccine fed strongly into vaccine-hesitant views and beliefs of our research participants. Distrust of healthcare and science institutions are accompanied by grievances related to the transparency of information and data about the COVID-19 vaccine development process. Our findings indicate that vaccine-hesitant individuals among minoritised communities were concerned that the development of the COVID-19 vaccine was “too fast”. Furthermore, some of our Black British, Black Caribbean and African American participants were wary that the vaccine trials have not taken into account possible reactions of Black populations to the vaccine before rolling it out. Our research participants associated the rapidity of vaccine development with insufficient research for the development of or trials for the vaccine before its approval. The perception that its development was rushed through further prompted a curiosity towards possible reasons that account for the urgency.
In cases when vaccine information and data sources seem compromised or insufficient, our participants show the tendency to ignore explanations on the basis of medical urgency and rather contemplate on the more threatening and salient aspects of the vaccines or vaccination programmes. Stories and reports about vaccine side-effects – short-term and long-term - took a toll on our research participants’ willingness to consider receiving a vaccine for an illness which they perceived as not being too threatening, especially for younger populations. To this end, this report also shows that our participants relied on other peoples’ stories and experiences with side-effects of the COVID-19 vaccine and other vaccines to inform their decision whether to refuse the vaccine or to take it due to peer or work pressure. In some cases, our research participants reported that side-effects can seem worse than the symptoms of COVID-19. Participants also tended to wait and see how the vaccine side-effects evolve over time, and how more people respond physiologically and physically to the COVID-19 vaccine.
T4. Spiritual and religious beliefs: Religious and spiritual beliefs inform vaccine hesitancy
Our findings also convey that religious and spiritual beliefs played a significant role in the vaccine-hesitant beliefs and ideas of minoritised communities. Our participants delineated that they would hesitate from taking the vaccine on the grounds that it was “a sin” to ingest harmful chemicals and that the vaccine was made of foetal cells, which contradicts a religious and Christian ‘pro-life’ stance. Some of our Muslim research informants also reported that they believed in the “power of prayer” and that Islam encourages the protection of one’s body and “something inserted in your body is not good for your health”. Overall, our Christian, Muslim and other religious participants reported that their religious and spiritual beliefs informed their vaccine decisions during the pandemic.
Many participants from minoritised communities also reported that they preferred natural remedies instead of man-made pharmaceutical drugs or vaccines. Some of our research participants highlighted that vaccines are not needed since they did not exist in times when people still managed to cope naturally with illnesses. Also, some of our participants identified the COVID-19 vaccine as “a DNA vaccine”, which would make genetic changes and damage the human body as created by God. These are examples of explicit religious beliefs affecting vaccine attitudes. Our findings also reveal instances where religious beliefs indirectly or implicitly affected participants’ stance on vaccines. For instance, some participants did not explicitly mention that religious beliefs prohibit them from receiving the vaccine, but rather stated that they refused the vaccine for unrelated reasons (e.g., side-effects), only to later mention their religiosity in the context of vaccination (when they were specifically asked about their religious beliefs). Aside from religious beliefs, non-religious spirituality, and strong beliefs in “natural remedies”, alternative and holistic medicine were noted among the preferences of some vaccine-hesitant participants in both countries, which impacted on the vaccine-hesitant beliefs of our research participants.
T5. Ineffective communication: Conflicting information from officials, mainstream media, and social media feed vaccine hesitancy
During our fieldwork, our research participants from minoritised communities indicated that they felt excluded from medical processes, belittled, and discriminated against. They found official medical and government advice confusing and inconsistent. Our research participants also reported what they perceived to be low-quality communication with governmental institutions and medical practitioners. There was a perceived lack of adequate information and data on the vaccine side effects, while the tone of official advice was perceived as being driven by a push to get the population vaccinated irrespective of possible side-effects or moral choices and responsibility. In addition, the lack of understanding of the mRNA technology and lack of trust of big pharmaceutical companies (in particular Pfizer) contributes to vaccine hesitancy. Vaccine-hesitant populations have also been mislabelled as “anti-vaxxers” and “conspiracy theorists” – terms which many participants disavowed. This further diminished the likelihood of participating in any kind of informed debate with vaccine-hesitant communities. Our findings show that some of the vaccine-hesitant individuals amongs minoritised communities would be willing to reconsider taking the COVID-19 vaccine if their concerns were adequately addressed through official health communication and public debate.
Our findings also indicate that anti-vaccine passport protesters in the UK viewed mainstream media, such as the BBC, as morally corrupt and as conspiring with political establishment institutions for the purposes of tyranny and control.
Our research participants within anti-vaccine protest movements reported that they actively resisted mainstream news sources, due primarily to their political interests.(16) One of the UK participants, who also protested, labelled mainstream media consumers as complicit, which is representative of a conspiratorial outlook. On the other hand, vaccine-hesitant participants who were not part of anti-vaccine protests were less averse to mainstream media in both countries. Due to exclusive official communication, divisive mainstream media coverage (even if this was perceived partly differently in the US) and the official labelling of their own vaccine communities as “anti-vaxx”, our informants formed a sense of heterogeneous but communal identity on their own close social networks online or in perceived safer physical spaces, such as the anti-vaccine passport protests or their church community.
We also show that our research participants, who were active in anti-vaccine passport protests, were most likely to avoid mainstream media and congregate on alternative social media platforms such as Telegram. In addition to alternative (and newer) social media platforms, evidence clearly shows the importance of YouTube videos for all research participants within and outside vaccine passport social movements in both countries. Our findings reveal that YouTube was widely used by vaccine-hesitant participants to obtain (as well as in some cases disseminate) health information during the pandemic. However, some of our research participants also perceived YouTube as a complicit platform due to the power of its suggestion algorithms and perceived breaches of impartiality. For this reason, some of our research participants reported that they navigated towards newer and smaller platforms such as Parler and Rumble, where these participants recounted that they shared their own views freely on the COVID-19 vaccine without being censored.
One of our findings is that members of various vaccine-hesitant communities connected with like-minded people and found them more trustworthy. Our findings show that vaccine-hesitant individuals among minoritised communities trusted online videos, documentaries, information, and data circulated on some of the legacy social media platforms such as Twitter as well as information and data disseminated on the COVID-19 vaccine and the pandemic on newer social media platforms. The tendency of our informants in coalescing with like-minded people on social media platforms in addition to the intrinsic design of social media platforms (i.e., their algorithms driving more interaction) play crucial roles in creating online echo-chambers.
Additionally, our findings from interviews and focus groups suggest that the anti-vaccine protesters among vaccine-hesitant groups were more likely to use Telegram. Our research uncovers that many of our interviewees, who were part of the anti-vaccine passport protests, coalesced around conspiracy theories and populist narratives, whilst moving in the direction of radicalisation. On the other hand, Telegram content came in contrast with beliefs and attitudes shared by our vaccine-hesitant participants among minoritised communities, who did not identify themselves with anti-vaccine protests. Our interviewees outside the anti- vaccine protests often criticised the protests. However, while the posts on Telegram highlighted an increased dehumanisation of outgroup members, our interviewees’ statements distressed the importance of tolerance to all types of vaccine voices. All these findings account for the diversity of reasoning, opinions, beliefs, social and political backgrounds, and political ideologies within vaccine-hesitant communities. Even if their purposes are different, the three Telegram channels that we analysed namely TRUTH PILLS, Covid Red Pills and Vaccine Injuries shared a similar tone when discussing mandates or protests. The negative sentiments about lockdowns and vaccine mandates and the feeling of discrimination were shared by both the Telegram channels and our interviews. Some of the themes and topics such as “side- effects”, “Bill Gates”, “children’s safety”, and the overarching themes of “personal freedoms” and “authoritarianism” were common to both data gathered through Telegram channels and the interviews and focus groups. A central theme across the evidence of these Telegram channels is that the messages invoked values of freedom and liberty and discussed the discontent of vaccine-hesitant individuals towards vaccine mandates. The messages around vaccine injuries, on the other hand, had an emotional and sensational tone. What differentiates the posts in Telegram from our interviews is the fact that one of the most popular topics about vaccines on Telegram is anti-vaccine mandate protests. For example, Covid Red Pills channel primarily aimed to inform their followers about national and international protests against vaccines.
We found out that the language of two Telegram channels namely TRUTH PILLS and Covid Red Pills contains populist dichotomies and radicalised calls to action. These channels also include more radicalised groups, such as “Alpha Men Assembly”, who meet regularly in physical spaces to practice military warfare tactics. The main difference between these two channels was that the UK channel TRUTH PILLS talked primarily about political and everyday issues in the UK, such as a situation about NHS during the pandemic or Boris Johnson’s public speech or action on the vaccine. Also, there were a lot of specific mentions of UK local protests and gatherings in this channel. In general, the TRUTH PILLS channel played a more organising role. However, the US channel Covid Red Pills talked more about US political issues such as Biden. Even though the US channel organised people by calling for local representatives in some messages, there was not a lot of grassroots organisation in terms of actually meeting in local parks or other public spaces. This is partly because the US users are from large cities in different states. With a few exceptions like calling people to attend protests, the US channel Covid Red Pills did less organising and shared more global protest news when compared to TRUTH PILLS.
The third Telegram channel we analysed was Covid Vaccine Injuries, which accounts for our aim to identify different types of Telegram channels on vaccine communication. We found out that the focus of this channel is on communicating information about injuries caused by vaccines. Our topic modelling findings of this channel show that the supposed symptoms and side-effects associated with the COVID-19 vaccine are diverse and include blood clots, myocarditis, heart attacks, death, and miscarriage. Almost all messages about the side-effects of the COVID-19 vaccine from this channel were accompanied by images or videos with emotional and sensational content. Some of these contents use descriptive storytelling in first person, or they associate incidents happening to famous individuals due to the COVID-19 vaccines. Some of the side-effects highlighted on this channel, such as blood clots and heart attacks, were also mentioned by our interviewees and focus group participants. These channels also deploy exaggerated claims and fear mongering and use language designed to trigger moral emotions such as anger and disgust which are known to inform dehumanisation, Our findings show that there is higher ideological homogeneity in Telegram channels, which is also related to the fact that only a small number of people moderate these Telegram channels and decide on what is shared there. Despite the low number of administrators on these channels, they are still significant as they are followed by thousands of other users. However, these moderators do not necessarily represent the vaccine-hesitant community entirely. On the other hand, our topic modelling analysis on Twitter posts shows that race and racism were present at the centre of vaccine conversations, shared using hashtags related to the COVID-19 vaccine and Black Lives Matter (BLM).
Our systemic analysis on these tweets shows that mandates were perceived as racist by the users who posted on these hashtags. This is primarily because the African American community was perceived as more vaccine-hesitant than other communities. The topic modelling on the posts shared on these hashtags reveal that the BLM organisation, at least in some parts of the US, held the view that vaccine mandates were racist and disproportionately impacting African Americans. This important issue was potentially overshadowed by louder groups of 1) anti-mandate activists, who viewed BLM as an important focus in their fights against vaccine mandates and, 2) far-right individuals, who saw vaccine mandates as leftist agendas that fell under the same umbrella as BLM and antifa.
Most notably, these findings emphasise the importance of having an intersectional approach towards vaccine hesitancy, which includes an analysis of the broader narratives and lived experience of vaccine-hesitant communities beyond the pandemic as well as the more specific vaccine communication about COVID-19 vaccine on social media platforms. In addition, our approach of analysing both interviews, focus groups and social media data reveals complementary findings. While the loudest voices on social media captured a strong anti-vaccine sentiment, findings from our interviews and focus groups were more nuanced and provide many additional reasons why people on the individual and community level may refuse to take the COVID-19 vaccine. Furthermore, conducting interviews and focus groups with vaccine-hesitant individuals within minoritised communities in the UK and US allowed us to hear and represent voices that were not necessarily represented in social media conversations about the vaccines.
T6. Medical experts: Lack of awareness and guidance regarding minoritised communities’ concerns
Our research also highlights biases and assumptions within medical communities about minority groups, which perpetuate mistrust based on historical unethical practices by dominant culture group members. Through our interviews with medical practitioners in the UK and US, we also aimed to understand the impact of patient-healthcare provider relationship in building trust and strengthening vaccine confidence. Our findings from our interviews with medical practitioners reveal that there were several difficulties medical professionals faced when discussing vaccine hesitancy with their patients during the pandemic. First, medical practitioners in our sample recounted that many vaccine-hesitant patients had the perception that the vaccine was insufficient to protect them from the virus and to stop transmission.
Second, our medical practitioner participants in the UK and US pointed that the belief among their patients that there was a high likelihood of experiencing mild symptoms if contracting COVID-19 was widespread. Furthermore, our medical practitioner research participants identified that unregulated posts on social media may have also negatively influenced their patients’ willingness to get vaccinated, especially considering that salient cases involving heavier side-effects are more visible online than the millions of cases with mild or non-existent side-effects. On the other hand, medical practitioners pointed out that people who better tolerated vaccine side-effects were more likely to encourage others to receive the vaccine.
Interestingly, our findings show that stories about the side-effects can also affect medical professionals’ decision to refuse a specific brand of vaccine, which was the case with one participant refusing Pfizer.
Our findings show that our medical practitioner participants also encountered further challenges from vaccine-hesitant patients who would trust their medical advice for treating other illnesses such as cancer, but not when it came to COVID-19.
Another theme frequently featured in patient-physician conversations, recounted by our medical practitioner participants, was vaccine hesitancy on the basis of religious beliefs. In addition, our professional participants believed that social conservative norms prohibiting vaccine uptake are passed down to younger generations in some communities. Furthermore, our findings reveal that some of our medical practitioner participants’ patients were suspicious of the profit motives of the pharmaceutical companies producing the vaccine, which came up in their interactions with their patients. Medical practitioners in our sample identified COVID-19 mutations, which make the illness less severe, as possible factors that further fuel vaccine hesitancy among patients.
The most frequently mentioned demographic group perceived by our medical practitioner participants to be vaccine-hesitant was Black, Asian, Middle Eastern, Native Americans and/or Gypsy and Traveller communities. When we asked the medical practitioners if they would say there are communities which on the whole are more prone to vaccine hesitancy, the majority of the US medical practitioners (five out of six) mentioned African American community and three out of six mentioned right-wing Trump supporters as the biggest vaccine hesitant groups in the US. Two medical practitioners also referred to religious groups and one mentioned the native Americans. British medical practitioners’ responses showed more discrepancy as they mentioned different demographic groups to be more prone to vaccine hesitancy: Out of eight participants, the majority (three participants) mentioned Black communities and another three participants mentioned white people including new age subculture, blue collar working people, and religious groups such as Muslims or Jehovah’s Witnesses followers/believers. Two participants mentioned South Asian communities, one participant mentioned Gypsy and Traveller communities.
When our medical practitioner participants were asked if they previously heard about any historical medical mistreatment of minoritised communities, the UK participants often responded to us with vague answers, reflecting their uncertainty about what exactly happened in the past. Medical practitioner 4, for instance, said that “yes, I heard of it in the past (here, interviewee refers to historical mistreatments in the UK), but I don’t know if it was a drug trial or what”. On the other hand, the US medical practitioner participants were more certain of their answers to this question, reflecting their knowledge of historical medical mistreatment in USA. US medical practitioner 4, for instance, mentioned “there is a definitive history of that happening within the United States”. US medical practitioner 5 also said “I think the African American population seems to be somewhat hesitant as well. You know, probably with good reason. And I don’t know if you’re familiar with the Tuskegee experiment with syphilis back in the day, and you know, not feeling in general like the government is doing what it should to promote equality among them, compared to Whites and other ethnic groups”.
Furthermore, medical practitioner participants working within the healthcare system in both countries were not aware of the existence of any kind of tailor-made guidelines of treating members of minoritised communities. Instead, our medical practitioner participants recounted that there are only ‘one-size-fits-all’ solutions and recommendations by the healthcare systems in these countries. In the absence of specific guidelines, some medical practitioners have taken it upon themselves to re-establish trust among minoritised communities by, for instance, choosing to receive the same brand of vaccine also offered to their patients. Such attempts signal trust in the safety of vaccines, which can help with the decision process of patients who fear side effects and are also cautious because of past discrimination or who suspect pharmaceutical companies of focusing on profit instead of patient safety. Our medical practitioner participants also reported taking the time to listen to patients’ concerns over vaccine side effects and addressing their hesitancy in counselling sessions.
However, some of the medical practitioner participants’ conceptualisations of vaccine hesitancy revealed a perceived homogeneous social group, which carried negative connotations rooted in the marker of “anti-vaxx”. As we put forward in the earlier parts of the report, most of our interviewees who were vaccine-hesitant did not want to be labelled as ‘anti-vaxx’ or ‘conspiracy theorists’. We acknowledged that naming vaccine-hesitant communities ‘anti-vaxx’ and imagining them as a homogeneous group hindered a genuine dialogue with and understanding of their individual or collective concerns related to vaccines. The moral concern for freedom from vaccine mandates was acknowledged by medical professionals to play a central role in vaccine hesitancy. Some participants believed that mandating the vaccine for healthcare professionals with penalties of job loss for non-compliance constitutes a form of discrimination. While this report primarily critically engages with the biases and prejudices of minoritised communities that are vaccine-hesitant towards the government, healthcare system and providers, it also unpicks the biases and prejudices of medical practitioners towards vaccine-hesitant communities as well as their reflection of what steps and approaches should be taken in healthcare systems in the UK and US for a better dialogue and trust between vaccine-hesitant communities and healthcare providers.
Policy implications and recommendations
Based on the 5 themes of T1- Racism and discrimination, T2-Liberty and freedom, T3-Side effects, T4-Religious beliefs, and T5-Medical experts in our findings, we suggest five strategic goals for policymakers to pursue (see Figure II). We believe these policies and strategy suggestions will help policymakers to address social inequalities and mistrust felt by minoritised communities, and guide policymakers in how to look to the future and shape the COVID-19 decade.
Figure 2: Policy recommendations
1. Acknowledge the bias and discrimination within healthcare institutions and biomedical models of health
We suggest that one of the most important entry points to reduce vaccine hesitancy in minoritised communities, is by building trust. The lack of responsibility for past medical malpractice is still present in the reasoning process of minoritised communities and being more transparent about these issues would help rebuild trust among these communities. Due to the prevalent theme of T1-Racism and discrimination, we recommend that governments and healthcare institutions in both the US and UK approach minoritised communities by acknowledging community-specific differences in health precautions and opportunities. Participants from historically minoritised communities in our sample reported that they were suspicious of the governments and public health institutions whose predecessors had discriminated against them. We have also found that public health initiatives surrounding the COVID-19 pandemic have treated all patients uniformly, which suggests a lack of awareness - or at best a lack of acting on the awareness - that different communities have different histories, everyday lived experience and needs. We suggest that future public health initiatives should lead with acknowledging social injustices and tailor their health strategies and approaches accordingly.
We propose that these changes need to be adopted at the individual level, for example, when patients inform their doctor about their pain, they are not dismissed due to historic, intentional, and discriminatory misconceptions, for this, educating the medical practitioners about historical malpractices is important. Our interviews with medical practitioners indicated a lack of formalised education and training on structural racism within healthcare. At the community level, community outreach initiatives including open forums and public workshops which will bring medical practitioners and minoritised communities are important; and at the societal level, this can be done through open acknowledgement of the government and healthcare institutions such as the NHS (UK) or healthcare providers (US) of the historic and ongoing mistreatment of racially minoritised communities specifically in the context of discussing the COVID-19 pandemic and vaccine programme. Only through building up these relationships and tackling these prevalent issues can the disparity of the impact of the pandemic on minoritised communities begin to be addressed, with the aim that should any future similar pandemic occur, these disparities are minimised and are addressed from the outset.
2. Prioritise building strong relationships between minoritised communities and healthcare institutions
Drawing on our findings from the themes of T1-Racism and discrimination, T4-Religious beliefs, and T5-Medical experts, we propose outreach initiatives such as open forums which take place within communities to disrupt normative expectations of unequal relationships that many of our participants described as characterising their interactions with healthcare practitioners. Where possible, these community outreach projects should include trusted members of communities, including religious leaders (T4), and medical experts (T5) to facilitate trust and rapport. Further, these open forums should be uncoupled from expectations of vaccine uptake - in other words, messaging from these initiatives should reduce reliance on vaccine rates. Instead, we recommend that they function as spaces where individuals feel that they can have open dialogues to discuss their concerns, beliefs, and experiences and receive responses without judgement or expectation that at the end of the conversation they will take the vaccine.
This would address the concerns raised by participants that they obtained much of the knowledge about the vaccine through personal research (e.g., online), because they felt that they could not hold these conversations with healthcare practitioners or in some of their immediate social networks due to potential stigmatisation. Through addressing the lack of procedures, guidelines, and strategies to approach minoritised individuals who are reluctant to vaccinate and ensuring that healthcare practitioners are aware of these specific resources, more formal support can be given to minoritised individuals who are concerned about the vaccine. Additionally, through building up guidelines surrounding the COVID-19 vaccine for minoritised communities, sources of information can be made more reliable and regulated by social media companies.
Resoundingly, our minoritised interviewees’ narratives suggest that the way to begin the long journey to earning their trust is twofold - through openly acknowledging the bias and discrimination within healthcare institutions and biomedical models of health, and through listening - and valuing - their lived experiences. This is particularly important to highlight as many of our medical practitioner participants in the UK, especially those from privileged and dominant cultural identities did not demonstrate an awareness of the systemic discrimination and racism of healthcare institutions, either historic or ongoing. Thus, these community outreach forums would also embed active anti-racism training and practices for healthcare practitioners. Our interviews also show that more minority representation among medical staff would also help improve engagement with the vaccine. Only through building up these relationships can the disparity of the impact of the pandemic on minoritised communities begin to be addressed, with the aim that should any future similar pandemic occur, these disparities are minimised and are addressed from the outset.
3. Acknowledge the agency and moral concerns of patients
Based on the themes of T2-Liberty and freedom, T4-Spiritual beliefs and T5-Ineffective communication, we suggest that the governments and healthcare institutions in both the US and UK approach minority communities by acknowledging their agency and moral concerns such as concerns for preventing harm, favouring one’s ingroup, or being fair to some communities only. For instance, our findings show that many people who oppose vaccine mandates do so while raising moral concerns for freedom. Fairly recently, moral psychologists have uncovered that some people seem to care more about their personal freedoms than others, and that they are more sensitive to potential violations of these freedoms.(17) (18) We have observed a relatively increased concern for personal freedoms in our vaccine-hesitant participants as well, especially within those who were also protesting vaccine passports and mandates.
While it is important to look at patients under the perspective of an aggregate of agents in order to model, control, and reduce the spread of the virus during a pandemic, it is also important to address each agent individually. Many participants felt the lack of a real debate on vaccine and vaccine passport mandates, that their concerns were not listened to, and felt excluded even from the superficial debate dividing patients into ‘good citizens’ and ‘conspiracy theorists’. When individuals who are highly concerned about protecting their personal freedoms are told that they have to receive/pressured into receiving a physically intrusive procedure (e.g., vaccine), they perceive this as violating their freedom, become morally outraged and oppose the mandate. We therefore recommend that public health communication strategies involved in future vaccine rollouts should also include messaging related to moral concerns, especially to the concern for individual freedoms. This is because concerns for personal freedoms are likely to negatively impact future public health initiatives as well.
4. Improve the way information and data are shared with publics
The theme of T3-Side effects and T4-Ineffective communication highlighted that a large portion of vaccine hesitancy was caused by fears of adverse effects of vaccines. Our findings reveal that our vaccine-hesitant participants tended to look for additional information on COVID-19 vaccines as they felt they received insufficient information from government institutions. We suggest that in future communications, additional transparency, and clarity in explaining side effects and how often they occur can be helpful especially in times of challenging historical moments, such as the COVID-19 pandemic. Governments and health organisations should also provide the public with clear and transparent information about the science behind vaccine development and vaccine efficacy.
We suggest that the UK and US governments and policymakers should partner with communications and information visualisation experts to develop effective, simple, and useful methods for communicating complicated health-related information. A large portion of our participants’ fears of the side effects were caused by anecdotes originated from personal, family members, or friends’ experiences. We suggest government communications to focus on 1) communicating the issues of relying on anecdotes, and 2) visualising information that communicates sample sizes. Furthermore, as storytelling is a powerful persuasion tool, we suggest messaging about vaccine benefits to focus on vivid individual stories presented by data visualisation, in addition to using statistics and numbers. Public health initiatives could also produce intuitive educational videos on the mRNA technology or use gamification to enhance the understanding of this technology.
5. Recognise the varied life experiences of vaccine-hesitant communities and avoid polarising discourse
Specially based on T5-Ineffective communications, as well as all the emergent theme within our study, we also recommend that public institutions including media companies adopt a language that does not stigmatise vaccine-hesitant individuals and communities for the social and medical problems of the COVID-19 pandemic. Vaccine mandates have quickly become a polarising issue leading many vaccine- hesitant individuals to hide their true concerns for fear of suffering social costs such as being shunned by their immediate social circles or financial costs such as losing their jobs. While public health initiatives were admittedly not designed to achieve these goals, such outcomes can be seen as side-effects of the current COVID-19 vaccine mandate. Future initiatives should therefore take patients’ estimated social costs into account.
Media companies should also avoid categorisations such as “anti vaxx” which divide society into two opposing poles between the vaccinated and anti-vaccinated. Generalising minority communities among vaccine-hesitant people with the term “anti-vaxx” prevents us from understanding the nuances of the personal experience that form their reservations and shape their decisions. Finally, governments may commission board game developers to create educational games aimed at recreating the unequal socio-economic and historic conditions faced by members from minoritised communities. In such games, individuals from different backgrounds, including medical practitioners and policy makers, would get the chance to familiarise themselves with the specific obstacles which minoritised communities face in accessing healthcare for instance, or in having to deal with neglect and discrimination.(19)
Conclusion
Through our interviews, focus groups, and social media data collected during the COVID-19 pandemic, we have identified significant variation in levels of mistrust not only towards the governments but also the healthcare systems and scientific advice of the day. We also encountered different factors that motivate hesitance of our interviewees over vaccines, depending on whether they are part of different ethnic, religious, cultural, or racial communities. Additionally, we found differences in levels of vaccine hesitancy of people that identify with the anti-vaccine protests and those who do not identify with them. We account for these variations as a factor of the specific lived histories, past legacies, and current discrimination which results in the unequal access to opportunities for minoritised communities. Our approach highlights the need for an intersectional perspective for designing public health policy in order to better account for the differential obstacles commonly faced by members of minoritised communities. We identified the central themes factoring into the decision of minoritised participants to refuse or delay receiving the vaccine, as well as contextual and structural factors reinforcing this outcome.
Taken together, our findings indicate that there is a varying level of mistrust towards the governments and healthcare institutions in the UK and US, especially due to historical malpractice and marginalisation as well as contemporary discriminatory practices and policies in the healthcare system and beyond. In this report, we show that this mistrust significantly informs vaccine beliefs and decisions of minoritised communities in these countries. Regaining a foothold in a shared understanding of cultural and generational traumas experienced by minoritised communities would allow policymakers to clearly identify obstacles faced exclusively by these communities and to correct them. This will undoubtedly go a long way toward rebuilding trust in state institutions and public health initiatives among these communities.
As observed in our social media data collected from Twitter and Telegram, users tend to rely on ‘personal research’ for COVID-19 related information, which places the burden to distinguish between misinformation and credible sources on people. Our findings show that misinformation about the COVID-19 vaccine often relied on highly emotive language and themes that make this content appealing for users. Our findings from interviews and focus groups also indicated that the anti-vaccine protesters among vaccine-hesitant groups were more likely to use Telegram. However, our report shows that Telegram content came in contrast with the vaccine beliefs and attitudes shared by our vaccine-hesitant participants among minoritised communities, who did not identify themselves with anti-vaccine protests. This additionally reinforces the need for an intersectional approach to study vaccine hesitancy, social inequalities and mistrust.
Our findings in this report also show that higher transparency and more detailed information about vaccine trials and associated side effects are needed in order to build, maintain, and recover trust across different minoritised communities that are vaccine-hesitant in the UK and US. Any lack of transparency regarding either negligible but widespread or serious but rare vaccine side effects could seriously impede roll-out efforts. On the other hand, not fully levelling with the population can be read as a sign of paternalism, fuelling mistrust as people may reasonably wonder why vaccine information is not more accessible and widespread. We also found out that an additional important aspect of efficient governance could be through effective health messaging between the government and citizens, aiming at recovery during the pandemic. Governments, public health initiatives, and policy makers contemplating future vaccine initiatives should consider promoting an informed debate regarding contrasting beliefs and attitudes of refusing the vaccine on moral grounds, such as due to a higher sensitivity to the issue of personal freedoms. Lastly, we argue that politicians, media companies, community faith organisations, and GPs play critical roles in leveraging relationships between medical practitioners and vaccine-hesitant minority communities and addressing their concerns.
References
Balibar, E. and Wallerstein, I. (1991), Race, Nation, Class: Ambiguous Identities, London and New York: Verso.
Edgerly, L., Toft, A., and Veden, M. L. (2011), ‘Social movements, political goals, and the May 1 marches: Communicating protest in polysemous media environments’, The International Journal of Press/Politics, 16(3), pp. 314-334.
Graham, J., Haidt, J., and Nosek, B. A. (2009), ‘Liberals and conservatives rely on different sets of moral foundations’, Journal of personality and social psychology, 96(5), pp. 1029-1046.
Iyer, R., Koleva, S., Graham, J., Ditto, P., and Haidt, J. (2012), ‘Understanding libertarian morality: The psychological dispositions of self-identified libertarians’, PLOS ONE, 7(8), pp. 1-23.
Jamison, A. M., Quinn, S. C., and Freimuth, V. S. (2019), ‘“You don’t trust a government vaccine”: Narratives of institutional trust and influenza vaccination among African American and white adults’, Social Science & Medicine, 221, pp. 87-94.
Johnston, J. (March 2020), ‘Matt Hancock insists ‘herd immunity’ not part of government’s plan for tackling coronavirus’, PoliticsHome, https://www.politicshome.com/news/article/matt-hancock-insists-herd-immunity- not-part-of-governments-plan-for-tackling-coronavirus [accessed 24/03/2022].
Kennedy, B. R., Mathis, C. C., and Woods, A. K. (2007), ‘African Americans and their distrust of the health care system: healthcare for diverse populations’, Journal of cultural diversity, 14(2), pp. 56-61.
Lentin, A. (2000), ‘Race’, Racism and Anti-Racism: Challenging Contemporary Classifications, Social Identities, 6(1), pp.91-106.
Marcelin, J. R., Swartz, T. H., Bernice, F., Berthaud, V., Christian, R., Da Costa, C., ... and Abdul-Mutakabbir, J. C. (September 2021), ‘Addressing and Inspiring Vaccine Confidence in Black, Indigenous, and People of Color During the Coronavirus Disease 2019 Pandemic’, In Open Forum Infectious Diseases (Vol. 8, No. 9, p. ofab417). US: Oxford University Press.
Niño, M. D., Hearne, B. N., and Cai, T. (2021), ‘Trajectories of COVID-19 vaccine intentions among US adults: The role of race and ethnicity’, SSM-population health, 15, pp. 1-8.
Nuriddin, A., Mooney, G., and White, A. I. (2020), ‘Reckoning with histories of medical racism and violence in the USA’, The Lancet, 396(10256), pp. 949-951.
Office for National Statistics (January 2022), Coronavirus and vaccination rates in people aged 18 years and over by socio-demographic characteristic and occupation, England: 8 December 2020 to 31 December 2021. https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthinequalities/bulletins/ coronavirusandvaccinationratesinpeopleaged18yearsandoverbysociodemographiccharacteristicandoccupa- tionengland/8december2020to31december2021 [accessed 24/03/2022].
Omi, M. and Winant, H. (2015), Racial Formation in the United States (3rd Edition), New York and Abingdon: Routledge.
Perkins K. and Wiley S. (2014), ‘Minorities’ in Teo, T. (ed.), Encyclopedia of Critical Psychology, (New York: Springer), https://doi.org/10.1007/978-1-4614-5583-7_188.
Peteet, B., Belliard, J. C., Abdul-Mutakabbir, J., Casey, S., and Simmons, K. (2021), ‘Community-academic partnerships to reduce COVID-19 vaccine hesitancy in minoritized communities’, EClinicalMedicine, 34, pp.1-2.
Platt, L. (November 2021), Why ethnic minorities are bearing the brunt of COVID-19. https://www.lse.ac.uk/ research/research-for-the-world/race-equity/why-ethnic-minorities-are-bearing-the-brunt-of-covid-19 [accessed 24/03/2022].
Sauda, E., Wessel, G., and Karduni, A. (2021), Social Media and the Contemporary City, Abingdon: Routledge.
Vox (2021) Glad You Asked, S2, E4. Available at: https://www.youtube.com/watch?v=YUbSpI0J9aQ&t=19s&ab_ channel=Vox [accessed 24/03/2022].
Wagner, E. F., Langwerden, R. J., Morris, S. L., Ward, M. K., Trepka, M. J., Campa, A. L., ... and Hospital, M. M. (2021), ’Virtual Town Halls Addressing Vaccine Hesitancy Among Racial/Ethnic Minorities: Preliminary Findings’, Journal of the American Pharmacists Association, 62(1), pp. 317-325.
- Platt, L. (November 2021), Why ethnic minorities are bearing the brunt of COVID-19. https://www.lse.ac.uk/research/research-for-the- world/race-equity/why-ethnic-minorities-are-bearing-the-brunt-of-covid-19 [accessed 24/03/2022].
- Office for National Statistics (January 2022), Coronavirus and vaccination rates in people aged 18 years and over by socio- demographic characteristic and occupation, England: 8 December 2020 to 31 December 2021. https://www.ons.gov.uk/ peoplepopulationandcommunity/ healthandsocialcare/healthinequalities/bulletins/coronavirusandvaccinationratesinpeopleaged 18yearsandoverbysociodemographiccharacteristicandoccupationengland/8december2020to31december2021 [accessed 24/03/2022].
- Wagner, E. F., Langwerden, R. J., Morris, S. L., Ward, M. K., Trepka, M. J., Campa, A. L., ... and Hospital, M. M. (2021), ’Virtual Town Halls Addressing Vaccine Hesitancy Among Racial/Ethnic Minorities: Preliminary Findings’, Journal of the American Pharmacists Association, 62(1), pp. 317-325.
- Niño, M. D., Hearne, B. N., and Cai, T. (2021), ‘Trajectories of COVID-19 vaccine intentions among US adults: The role of race and ethnicity’, SSM-population health, 15, pp. 1-8.
- Peteet, B., Belliard, J. C., Abdul-Mutakabbir, J., Casey, S., and Simmons, K. (2021), ‘Community-academic partnerships to reduce COVID-19 vaccine hesitancy in minoritized communities’, EClinicalMedicine, 34, pp.1-2.
- Omi, M. and Winant, H. (2015), Racial Formation in the United States (3rd Edition), New York and Abingdon: Routledge.
- Lentin, A. (2000), ‘Race’, Racism and Anti-Racism: Challenging Contemporary Classifications, Social Identities, 6(1), pp.91-106.
- Balibar, E. and Wallerstein, I. (1991), Race, Nation, Class: Ambiguous Identities, London and New York: Verso.
- Perkins, K. and Wiley, S. (2014), ‘Minorities’ in Teo, T. (ed.), Encyclopedia of Critical Psychology, (New York: Springer), https://doi. org/10.1007/978-1-4614-5583-7_188.
- Sauda, E., Wessel, G., and Karduni, A. (2021), Social Media and the Contemporary City, Abingdon: Routledge.
- Kennedy, B. R., Mathis, C. C., and Woods, A. K. (2007), ‘African Americans and their distrust of the health care system: healthcare for diverse populations’, Journal of cultural diversity, 14(2), pp. 56-61.
- Jamison, A. M., Quinn, S. C., and Freimuth, V. S. (2019), ‘“You don’t trust a government vaccine”: Narratives of institutional trust and influenza vaccination among African American and white adults’, Social Science & Medicine, 221, pp. 87-94.
- Nuriddin, A., Mooney, G., and White, A. I. (2020), ‘Reckoning with histories of medical racism and violence in the USA’, The Lancet, 396(10256), pp. 949-951.
- Marcelin, J. R., Swartz, T. H., Bernice, F., Berthaud, V., Christian, R., Da Costa, C., ... and Abdul-Mutakabbir, J. C. (September 2021), ‘Addressing and Inspiring Vaccine Confidence in Black, Indigenous, and People of Color During the Coronavirus Disease 2019 Pandemic’, In Open Forum Infectious Diseases (Vol. 8, No. 9, p. ofab417). US: Oxford University Press.
- Johnston, J. (March 2020), ‘Matt Hancock insists ‘herd immunity’ not part of government’s plan for tackling coronavirus’, PoliticsHome, https://www.politicshome.com/news/article/matt-hancock-insists-herd-immunity-not-part-of-governments-plan-for-tackling-coronavirus [accessed 24/03/2022].
- Edgerly, L., Toft, A., and Veden, M. L. (2011), ‘Social movements, political goals, and the May 1 marches: Communicating protest in polysemous media environments’, The International Journal of Press/Politics, 16(3), pp. 314-334.
- Graham, J., Haidt, J., and Nosek, B. A. (2009), ‘Liberals and conservatives rely on different sets of moral foundations’, Journal of personality and social psychology, 96(5), pp. 1029-1046.
- Iyer, R., Koleva, S., Graham, J., Ditto, P., and Haidt, J. (2012), ‘Understanding libertarian morality: The psychological dispositions of self-identified libertarians’, PLOS ONE, 7(8), pp. 1-23.
- For an example, please see this video: Vox (2021) Glad You Asked, S2, E4. Available at: https://www.youtube.com/ watch?v=YUbSpI0J9aQ&t=19s&ab_channel=Vox [accessed 24/03/2022].
Summary
- Published
© The authors. This is an open access publication licensed under a Creative Commons Attribution-NonCommercial- NoDerivs 4.0 Unported License
To cite this report: British Academy (2022), "Medicine is still against Black people": Mapping and visualising intersections of social inequalities, community mistrust, and vaccine hesitancy in online and physical spaces in the UK and US, The British Academy, London
- DOI doi.org/10.5871/c19-recovery/O-O-B-A-O-A-KN-F-W-D-M-A-M-F (Opens in a new window)