COVID and the Coalfield: Vaccine Hesitance in Wales and Appalachia
COVID-19 Recovery: Building Future Pandemic Preparedness and Understanding Citizen Engagement in the USA and UK
By Christopher W N Saville, Robin Mann, April M. Young and Daniel Thomas
Download PDF report
- Published by
- The British Academy
- Year
- 2022
- Pages
- 15
Welsh language edition
A welsh language edition of this summary is also available.
About the authors
Dr Chris Saville is a Clinical Lecturer at Bangor University. Dr April Young is an Associate Professor in the Department of Epidemiology at the University of Kentucky. Professor Daniel Thomas is a Consultant Epidemiologist at Public Health Wales. Dr Robin Mann is a Senior Lecturer in Sociology at Bangor University and Co-Director of the Wales Institute of Social and Economic Research, Methods and Data (WISERD).
Acknowledgements
The authors would like to thank the British Academy for generously funding this work, particularly Flora Langley and Hugo Clarke who were very helpful and supportive throughout. Secondly, the authors are very grateful to Aidan Bark-Connell and Stella Gabuljah, the qualitative interviewers.
They accomplished an extremely ambitious set of interviews on a very short timeline and should be very proud of their work. Thirdly, the authors would like to thank the stakeholder advisers for all of their invaluable input: Ryan Jones from the Coalfields Regeneration Trust, Scott Lockard from Kentucky River District Health Department, Ashley Gould from Public Health Wales, and all those who attended workshops or met with the authors separately.
Fourthly, the authors would like to thank Fred Barber, Jacqie Boggess, Sam Leach, and Vladimír Sedláček at The Decision Company, and Lukas Paleckis,
Adam McDonnell, and Charlotte Smith at YouGov for their wonderful work on the fieldwork. Finally, the authors would like to thank the survey respondents and interviewees for their participation and for placing their trust in the project.
About the COVID-19 Recovery: Building Future Pandemic Preparedness and Understanding Citizen Engagement in the USA and UK Series
The programme is the result of a partnership between the British Academy, the Social Sciences Research Council (SSRC) and the Science & Innovation Network in the USA (SIN USA) to award funding to ten transatlantic studies focusing on UK-US COVID-19 vaccine engagement. It follows a pilot study exploring levels of vaccine engagement in four locations across the US and UK, while the larger programme was expanded to study multiple locations. The programme was funded by the UK’s Department for Business, Energy and Industrial Strategy.
Every little boy’s ambition in my valley was to become a miner There was the arrogant strut of the lords of the coal face One could stand on street corners and look at the posh people pass with hostile eyes Insulting were these cold looks, because they were the kings of the underworld
Richard Burton
Oh come all you young fellers so young and so fine Seek not your fortune in a dark dreary mine It’ll form as a habit and seep in your soul Till the stream of your blood runs as black as the coal
Merle Travis – ‘Dark as a dungeon’
Introduction
The impact of the COVID-19 pandemic has been felt especially keenly in disadvantaged communities, demonstrating what social epidemiologists call a social gradient in outcomes. (1) Social gradients have been observed across the range of outcomes, from infections to deaths,(2) and since vaccines for COVID-19 became available, we have seen a social gradient in their uptake, (3) which risks further entrenching health inequalities.
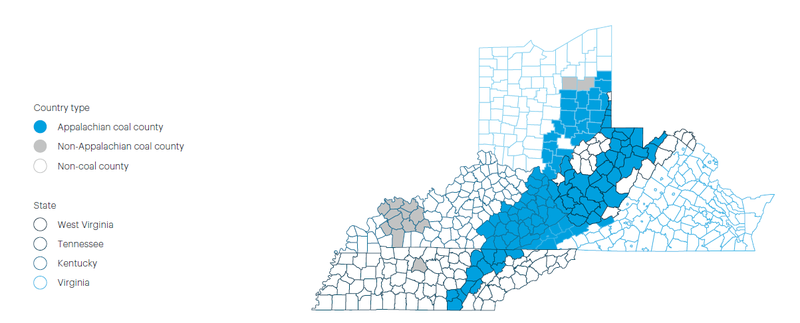
Although a useful shorthand, the concept of social gradients can ignore the specific contexts of particular types of disadvantaged communities. Not all disadvantaged communities are alike. This report focuses on COVID-19 vaccine uptake in the coalfield regions of Wales (Figure 1) and Central Appalachia (Figure 2). These communities share a common experience of industrialisation and deindustrialisation,(4) which has led to health, social, and economic inequities that endure to the present day.(5)
The decline of the coal industry from the second half of the twentieth century to the early twenty-first has been economically devastating for the coalfields of South Wales (6) and Central Appalachia.(7) As well as being a source of well-paying jobs, the mines were anchor institutions and much of civil society in these areas – unions, miners’ halls, choirs, etc. – depended on them. The mining industry’s decline has weakened civic society and the broader social fabric of these areas. Such social connections have been shown to be related to a wide range of health outcomes,(8),(9) and their decline is likely a contributing factor to the health inequalities we see today.(10) Social science research suggests that social trust is lower in coalfield areas of the UK,(11) perhaps due to the long and bitter history of industrial disputes between the miners and the UK Government. Similarly, there is evidence that industrial disasters in Appalachia have led to lower social trust.(12) This may have contributed to structural vulnerabilities for vaccine hesitancy and lower compliance with public health measures (13) in these areas.
For this project, we conducted two large-scale surveys in Wales (4187 respondents) and the states overlapping with Central Appalachia (4864 respondents from Kentucky, Tennessee, Virginia, Ohio, and West Virginia). These surveys asked for respondents’ vaccination status, views on COVID-19, economic status, social lives, and political views. The surveys were followed up with a set of 36 in-depth qualitative interviews with vaccinated and unvaccinated residents of the two coalfields, to deepen our understanding of people’s views on vaccination. We used the qualitative interviews to identify themes and present our findings under these themes below.
Figure 1. Extent of historical coal mining in Wales
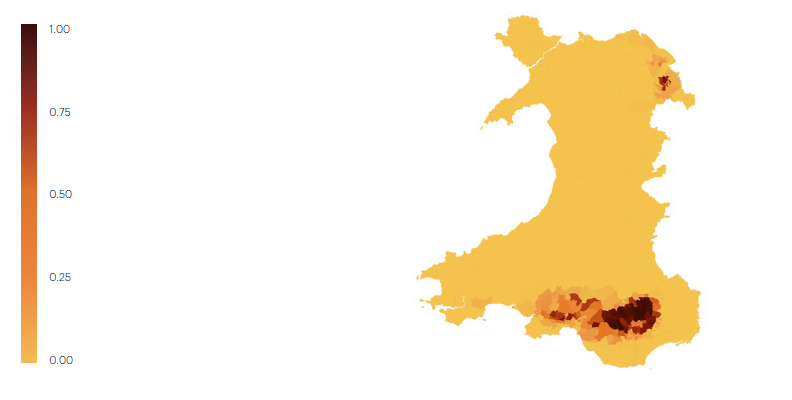
Figure 2. Coal counties in the US states overlapping with Central Appalachia
Vaccination and attitudes towards it
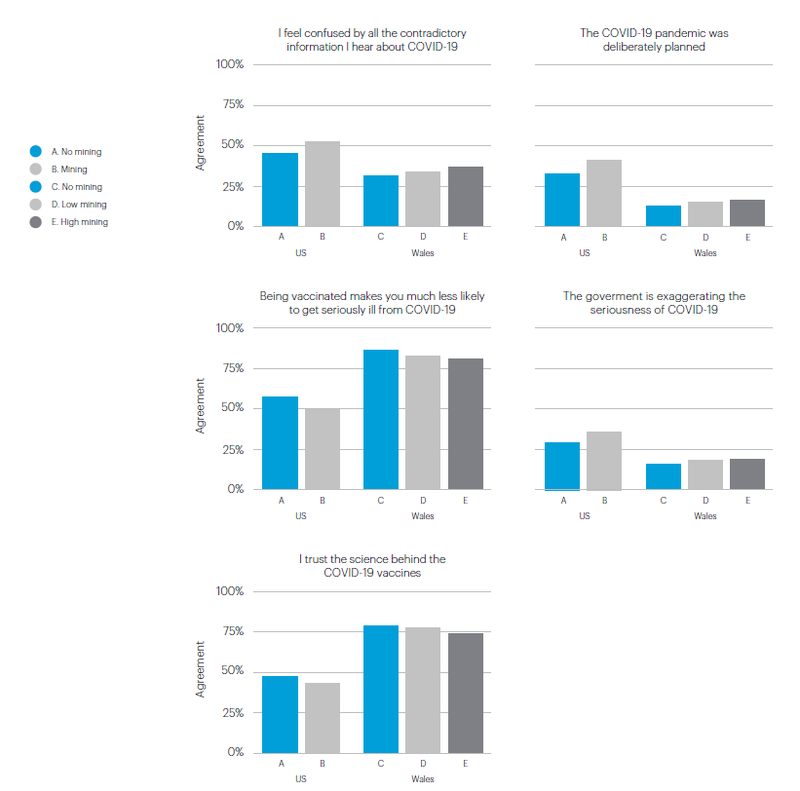
We found higher levels of vaccine hesitance and suspicion towards official accounts of the pandemic in coalfield areas, compared to non-coalfield areas (see Figure 3). Respondents living on the coalfields in both countries were less likely to agree that the vaccines protected people against COVID-19 or that they trusted the science behind the vaccines. They were likely to express confusion with contradictory information they received about COVID-19, believe that the government was exaggerating the seriousness of COVID-19, and agree that the pandemic had been deliberately planned.
Figure 3. Rates of agreement with selected statements about COVID-19 in coalfield and non-coalfield areas of Appalachia and Wales
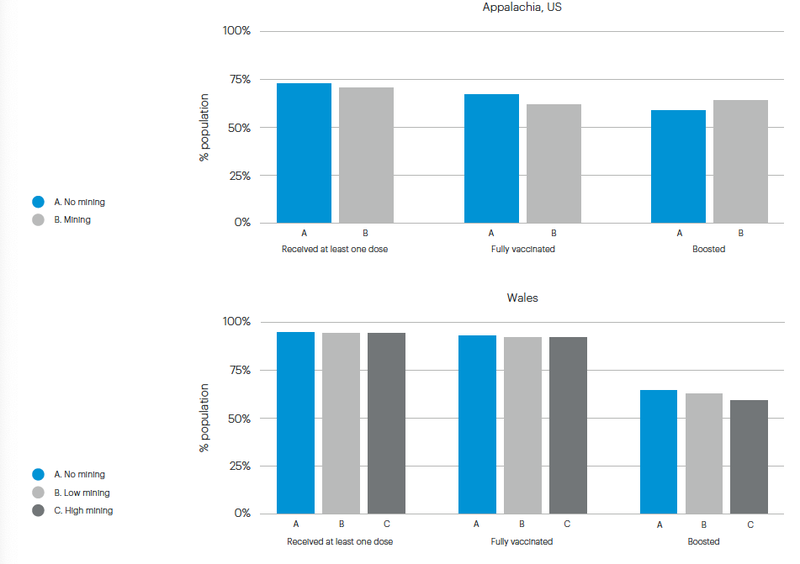
In our US sample, these attitudes were accompanied by a lower rate of reported vaccination in coalfield areas, but in Wales vaccination rates were equivalent in coalfield and non-coalfield areas, with the exception of booster dose rates, which were lower on the coalfield (Figure 4). This represents a striking policy success in Wales – our data suggest that a real risk of lower vaccine uptake in coalfield areas was averted. However, we would counsel against complacency here. The conditions for vaccine hesitancy exist in coalfield Wales and people’s trust in the vaccination campaign on this occasion should not be taken for granted.
Figure 4. Vaccination rates by coalfield status in the states overlapping with Central Appalachia and Wales.
The interviews reflected this. Vaccinated interviewees mentioned doubts on several occasions:
I don’t know if I was convinced like yes, I trusted it, I trusted it as much they could be trusted […] perhaps down the line there may be an enduring side effect. Who knows? I don’t know, nobody knows
Wales, vaccinated, male, 60s, retired
Material circumstances and experiences of the pandemic
We found lower vaccination rates in participants on lower incomes and in those who reported worsening finances during the pandemic. Respondents in the US who lost their jobs during the pandemic were also less likely to be vaccinated, while people on the Welsh coalfield who were furloughed from their jobs showed signs of lower vaccination rates. Economic distress, both related to changes during the pandemic and longer term hardship appeared to be risk factors for being unvaccinated. In some cases, this association was particularly strong on the coalfield: respondents from coalfield areas of Wales who reported worsening household finances were especially likely to be unvaccinated. Interviewees showed a clear awareness of the economic challenges facing their local communities: several respondents in Appalachia quoted poverty statistics fluently. There was some scepticism from vaccinated interviewees about the link between poverty and vaccination decisions:
I don’t think there is a link to poverty. I think in some cases, poverty is also equated to [being] uneducated, so I think that the being uneducated and thinking that everything that they hear from the news, the mainstream media is the link but just being the poverty itself, I don’t think there is a link
Appalachia, vaccinated, female, 60s, retired
However it was striking that several unvaccinated interviewees brought up the financial and occupational hardship they had suffered during the pandemic:
Since Covid, my husband’s hours have decreased […] he has lost some hours, so has lost money so we have lost money, so we’ve been struggling. Covid has hurt us bad…
Appalachia, unvaccinated, female, 40s, not working
We were having food parcels from school that were pretty dire and discretionary assistance fund. I was getting Universal Credit [the UK’s new welfare system] erm, but I think I was having about £450 a month coming in with Universal Credit. So if I had the mortgage then I would have completely lost my house, you know I didn’t have it.
Wales, unvaccinated, female, 40s, working
Belonging, isolation, and participation
Those who were unvaccinated, both in the surveys and the interviews, often appeared disconnected from the communities in which they lived. They were less likely to report being a member of various organisations, such as sports clubs, trade unions, and social clubs; and also less likely to report feeling a sense of belonging to their communities. These associations were particularly strong in coalfield areas in Appalachia. Such measures of social capital have long been associated with health outcomes,(14) and low individual social capital in areas which otherwise have a strong sense of community is especially negatively associated with health.(15)
In the Welsh survey, those who identified as Welsh were more likely to be vaccinated the greater the extent of historical mining where they lived, while the reverse was the case for those who did not identify as Welsh or those who specifically identified as English. This again pointed to those who are less integrated into their local communities being less likely to be vaccinated.
Differences between vaccinated and unvaccinated people in terms of how integrated they were into their communities was a theme echoed in the interviews. Vaccinated interviewees generally presented as feeling part of the fabric of their communities:
Yes, I belong here. This is my county. This my county. Yes I care about our community”
Appalachia, fully vaccinated, female, 60s, retired
Non-vaccinated interviewees, in contrast, appeared more likely to be socially isolated in various respects. Many described living alone, or with elderly parents. Many reported little in the way of participation in wider community life, socially or culturally:
…until all the lockdown stuff happened, and then the friends I did have around here moved away for various reasons and have never come back, so yeah, so I am in, well, I’m kind of in a more isolated position now than I was before, because I don’t really have anybody now. So it’s just as well I’m relatively happy with my own company.”
Wales, unvaccinated, female, 50s, working
In the interviews, it appeared that unvaccinated respondents tended to fall into one of two groups: Those who were socially isolated, as described above, and a second group who appeared to be firmly rooted in their communities, with what sociologists would call high bonding social capital, but mistrustful of the authorities and their account of the pandemic. Thus, although social isolation appeared to be associated with being unvaccinated, this profile did not apply across the board. The following quote illustrates one respondent’s account of her community’s approach to lockdown rules:
The household bubbles, I remember the first Christmas and we were supposed to be limiting the amount of people coming in and out of our house and my neighbours already said that they were gonna have lots of people in their house, and I was obviously gonna have my close family up here anyway. So I think everybody in the street kind of made a pact that we weren’t gonna grass each other up.”
Wales, unvaccinated, female, 40s, working
Trust, politics, and information
Unvaccinated participants expressed lack of trust in government, media, and people in general. This was a common theme in both the surveys and interviews.
In the surveys, trust in the US Federal government was particularly important on the Appalachian coalfield, while trust in the Welsh Government was more
important than trust in the UK Government on the Welsh coalfield. In Wales, trusting people one knew personally was a powerful positive predictor of being vaccinated, while in the US this relationship was weak to non-existent. This could be interpreted as reflecting weaker social norms for vaccination in the US compared to Wales.
It could be also be interpreted as reflecting different sources of social pressure pushing in different directions in the US, while social pressure was primarily towards vaccination in Wales.
The theme of trust and mistrust was reflected in the interviews:
Pauses then sighs] I just don’t trust it. I just don’t trust it. I’m just one of those backward hillbillies that doesn’t trust no one... I feel like we need a longer testing period... And you’re sitting there thinking she’s crazy right now…
Appalachia, unvaccinated, female, 40s, not working
There were lower rates of vaccination among survey respondents who voted for Donald Trump in the US and those who planned to vote for Reform UK and, to a lesser extent, the Green Party in Wales. Rates of vaccination were lower for those who voted leave in the UK’s referendum on European Union membership than those who voted remain. Non-voters were also more likely to be unvaccinated, echoing
our findings that those who are disconnected from wider society are less likely to be vaccinated. In Wales, those who expressed ‘devosceptic’ or hostile attitudes towards Welsh devolution were also less likely to be vaccinated. It was unclear whether
this relationship represented a natural alignment between the values underlying devoscepticism in Wales and vaccine hesitance,16 or whether this was simply contingent on the Welsh Government’s more cautious approach to the pandemic than that of the UK Government in England.
The interviews echoed this theme, with many vaccinated respondents praising the Welsh Government response, while some unvaccinated respondents favoured the English approach:
I know Drakeford [the First Minister of Wales] has had a lot of negative press with how he’s dealt with things, but personally I agree with what he’s done and he’s been cautious and, as far as I’m aware, there’s not been nepotism as there has been in the UK Government. I have far more respect for Welsh Government than UK government.
Wales, vaccinated, female, 40s, employed part-time
When asked whether the Welsh or English pandemic response had been better] England, because they have had a lot more freedom than we have in Wales, and if you look at the charts where the cases and the deaths, and what have you, they pretty much follow exactly the same trajectory, so, to me, all of this stuff has achieved nothing but division, hostility, intimidation, anxiety; all sorts of negatives”
Wales, unvaccinated, female, 50s, working.
Some unvaccinated interviewees, however, were just as suspicious of the UK Government’s position:
Well I don’t think Boris’s parties and things made it look like they were worried about Covid, they looked quite relaxed and happy in those parties, which is fine, fair enough for ‘em. But if it was so bad, then surely they would’ve been worried about taking things back to their own families and possibly killing their own families off because they’ve contracted Covid after a work party, so they obviously weren’t that worried about it, they want all of us to be worried about it.
Wales, unvaccinated, female, 40s, working
Policy implications
Our results suggest the following priorities for policymakers:
Explore ways to reach out to socially disconnected people
The vaccination campaign has been supported by wider civil society. Perhaps partly for this reason, many of those who remain unvaccinated are people who are disconnected from their local communities. In Appalachia, this association is particularly strong on the coalfield. Policymakers need to find ways to reach these people. Part of the solution may involve the means used to speak to them. Part of this may be more about the messaging used – encouraging people to help protect their communities may be less persuasive to those who do not feel part of these communities.
Our research also shows that people’s identities may be relevant for how they respond to public health advice. In Wales, the vaccination campaign was somewhat less successful among those sceptical of Welsh devolution. Potentially these groups may benefit from specific messaging (and carefully chosen messengers) to boost uptake.
Protect and build social capital as a matter of pandemic preparedness
People’s connections to one another and their communities are an important source of resilience and this has been confirmed by COVID-19. We recommend that policymakers regard the renewal and maintenance of community social capital as part of pandemic and disaster preparedness. Our neglect of our social infrastructure over recent years now looks complacent. Cost-benefit analyses of investment in local community social capital should price in not just the returns on health and wellbeing in ‘normal’ times, but also the extent to which we will be forced to depend on this social infrastructure in times of crisis.
Due to the long period of social distancing, and potentially the effects of experiencing a pandemic on one’s social attitudes,17 the last few years may have taken a further toll on social capital and post-pandemic rebuilding should include efforts to repair important components of our social fabric.
Take seriously the evidence of latent vaccine hesitance on the Welsh coalfields
Although the vaccination campaign in Wales was a success, our work shows that this was not inevitable and we should take seriously the latent hesitancy towards vaccines apparent in coalfield Wales. People’s trust in public health must be constantly re-earned and should not be taken for granted.
Build links between practitioners, researchers, and policymakers in different coalfield regions
In the course of this project we have launched a new collaboration between researchers and practitioners in Wales and Appalachia, and in doing so have found striking parallels between our two areas. Stakeholders in the two areas face similar social, economic, and public health challenges and there is considerable potential to learn from one another. We had a great deal of interest in our dissemination workshop event, bringing together practitioners and policymakers on the two coalfields. We believe that there are exciting opportunities for public health cooperation in the future.
Conclusion
Coalfields have important structural vulnerabilities for vaccine hesitancy. These risks have been realised in Appalachia but latent vaccine hesitancy also remains a longer- term risk on the Welsh coalfield. Many of the socio-demographic factors predicting being unvaccinated were especially predictive on the coalfield, such as social isolation and experiencing worsening household finances during the pandemic, speaking to the particular urgency of these issues in coalfield communities.
Many of the great successes of the pandemic – people’s preparedness for common sacrifice and the vaccination campaigns – have relied in no small part on social capital and community solidarity. This pandemic has also exposed some of the holes in our social fabric. It is important to recognise the value of this social capital for public health in the future. Work is needed to renew it and this need appears particularly pressing on the coalfield.
Citations
- Marmot, M, The Health Gap: The Challenge of an Unequal World.
- Kontopantelis et al., ‘Excess Deaths from COVID-19 and Other Causes by Region, Neighbourhood Deprivation Level and Place of Death during the First 30 Weeks of the Pandemic in England and Wales’.
- Perry et al., ‘Inequalities in Coverage of COVID-19 Vaccination’.
- Bowen et al., ‘An Overview of the Coal Economy in Appalachia’; Hudson and Beynon, The Shadow of the Mine: Coal and the End of Industrial Britain.
- Riva et al., ‘Coalfield Health Effects’.
- Hudson and Beynon, The Shadow of the Mine: Coal and the End of Industrial Britain.
- Zipper and Skousen, Appalachia’s Coal-Mined Landscapes.
- Klinenberg, Heat Wave: A Social Autopsy of Disaster in Chicago.
- Saville, ‘Estimating Ecological Social Capital Using Multi-Level Regression with Post-Stratification’.
- Shucksmith et al., ‘Health Inequalities in Ex-Coalfield/Industrial Communities’.
- Abreu and Jones, ‘The Shadow of the Pithead’.
- Scott, Westgate, and McSpirit, ‘The Long-Term Effects of a Coal Waste Disaster on Social Trust in Eastern Kentucky Updated’.
- Saville and Thomas, ‘Social Capital and Geographical Variation in the Incidence of COVID-19: An Ecological Study’.
- Kawachi, ‘Social Capital and Community Effects on Population and Individual Health’.
- Saville, ‘Not Belonging Where Others Do’.
- Henderson and Jones, Englishness.
- Aassve et al., ‘Epidemics and Trust’.
Summary
- Published
© The authors. This is an open access publication licensed under a Creative Commons Attribution-NonCommercial- NoDerivs 4.0 Unported License
To cite this report: British Academy (2022), Covid and the Coalfield: Vaccine Hesitance in Wales and Appalachia, The British Academy, London
- DOI doi.org/10.5871/c19-recovery/C-S-R-M-A- Y-D-J (Opens in a new window)