Bridging the Vaccination Gap: Policy Opportunity
COVID-19 Recovery: Building Future Pandemic Preparedness and Understanding Citizen Engagement in the USA and UK
By Marie Juanchich, Hazel Sayer, Claire Oakley, Louis Goffe, Cara Booker, Wandi Bruine de Bruin, Carly Meyer, Tim Chadborn, Miroslav Sirota, Gaelle Vallee-Tourangeau, Dawn Holford and Reed Wood
Download PDF report
- Published by
- British Academy
- Year
- 2022
- Pages
- 22
About the authors
Dr Marie Juanchich is Associate Professor in Psychology at the University of Essex. Mrs Hazel Sayer is a Research Assistant and PhD student. Mrs Claire Oakley is a Research Assistant and PhD student. Dr Louis Goffe is a Research Associate at the Behavioural Science, Population & Health Sciences Institute at Newcastle University. Dr Cara Booker is Research Fellow and Graduate Director at the University of Essex. Professor Wandi Bruine de Bruin is Professor of Public Policy, Psychology and Behavioral Science at the University of Southern California. Dr Carly Meyer is Research Fellow, NIHR Policy Research Unit Behavioural Science at University College London. Dr Tim Chadborn is Head of Behavioural Insights and Evaluation Lead at the Department of Health and Social Care. Dr Miroslav Sirota is Associate Professor in Psychology at the University of Essex. Professor Gaelle Vallee- Tourangeau is Professor of Behavioural Science and Director of Research and Enterprise at Kingston University. Dr Dawn Holford is Senior Research Associate, School of Psychological Science at the University of Bristol. Dr Reed Wood is Associate Professor at the Department of Government at the University of Essex.
Acknowledgements
The authors are very grateful to: Dr Andrew Parker, Senior Behavioral and Social Scientist; Faculty, Pardee RAND Graduate School; Dr Ana Wheelock Zalaquett, ONS, Researcher Associate, Imperial College London; Dr Ben Taylor, Deputy Director, Open Innovation Team of the Cabinet Office; Marianna Baggio, PhD, Policy Analyst EU Policy Lab, European Commission; The Public and Patient Involvement and Engagement Panel Strategy Group of the National Institute for Health Research
About the COVID-19 Recovery: Building Future Pandemic Preparedness and Understanding Citizen Engagement in the USA and UK
The programme is the result of a partnership between the British Academy, the Social Sciences Research Council (SSRC) and the Science & Innovation Network in the USA (SIN USA) to award funding to ten transatlantic studies focusing on UK-US COVID-19 vaccine engagement. It follows a pilot study exploring levels of vaccine engagement in four locations across the US and UK, while the larger programme was expanded to study multiple locations. The programme was funded by the UK’s Department for Business, Energy and Industrial Strategy.
Summary of policy opportunities
To increase vaccination uptake
1. Inform and educate people about the safety and effectiveness of the COVID-19 booster. Break down the data for men and women.
2. Debunk misinformation about vaccine risk and benefits wherever possible. Vaccination was a politically divisive topic, with more conservative voters being reluctant to be vaccinated (especially in the US, but also in the UK). To counteract this tendency, we recommend:
3. Support and promotion of vaccination should come from leaders across the political spectrum and explicitly refer to the recommendations of health experts (who are judged more trustworthy). In particular, Conservative leaders should make additional efforts to ensure a pro-vaccination message reaches their supporters to reduce and ultimately close the political divide in vaccination.
For example: “The Covid vaccine is safe and effective. The World Health Organization is clear on this matter and strongly recommend that we all get vaccinated when our turn comes”.
To tackle vaccine hesitation in ethnic minority groups in particular
4. Raise awareness that ethnic minority groups are at higher risk from COVID-19.
Inform people that those people from ethnic minority groups in the UK and the US are at higher risk from COVID-19: Provide a clear breakdown about the risk of infection, hospitalisation, and death across groups using icon arrays.
5. Provide autonomy-supportive messaging.
Use health messaging that empowers people to make decisions, offering them autonomy and the freedom to choose. Feeling empowered will be beneficial to all, especially people from ethnic minority groups (e.g., “Here is the information about the vaccine (…). We trust you will make the right decision”).
6. Provide control over the vaccination process.
For example, give people the opportunity to select which vaccine they can get, who will deliver the vaccine or where it will take place. Highlight how being vaccinated provides people with more control over their life as it reduces their risks of infection and their risk of infecting others (e.g., “Take back control and get your booster today”).
7. Provide inclusive information about the vaccine.
For example, clarify the breakdown of people’s ethnic backgrounds in the vaccine trials when communicating about vaccine effectiveness and vaccine safety.
8. Highlight positive vaccination social norms.
Especially within groups with a lower-than-average vaccination rate: “Most people in your community recognise the positive value of the COVID-19 booster vaccine and are vaccinated, do it too”.
To foster trust in vaccination invitation messages and increase booking intention
People find typical text message vaccination invitations untrustworthy. To elicit trust and increase booking intention:
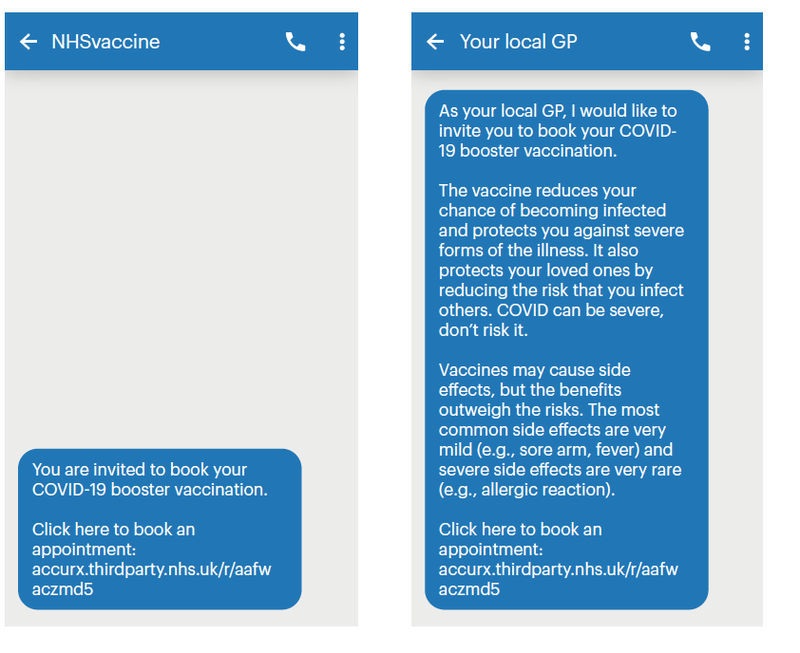
9. Use trustworthy message senders such as GP/family physicians.
Make the message warmer and highlight the competence of the source. For example: “As your local GP and a health expert who cares for the local community,
I would like to invite you to book your COVID-19 booster vaccination.” Instead of what is currently used: “You are invited to book your COVID-19 booster vaccination.”
10. Text messages should highlight vaccine benefits and risks
Messages should focus on the benefits for the self and the local community. For example: “The vaccine reduces your chance of becoming infected and protects you against severe forms of the illness. It also protects your loved ones by reducing the risk that you infect others. Covid can be severe, don’t risk it.
Vaccines may cause side effects, but the benefits outweigh the risks. The most common side effects are very mild (e.g., sore arm, fever) and severe side effects are very rare (e.g., allergic reaction).”
11. Use vaccination booking web links that are easy to read and identify a clear and trusted website host.
For example, use the fluent link where the NHS is easier to be identified: ‘https://vaccine-booking.nhs.uk’ instead of the currently used ‘https://accurx.thirdparty.nhs.uk/r/aafwaczmd5’.
Executive summary
Research approach
This research was conducted by an interdisciplinary team led by Dr Juanchich and funded by the British Academy. The research investigates why people agree or not to take the COVID-19 vaccine booster in the UK and the US. We focus in particular on what may cause vaccination uptake differences across ethnic groups to inform future public health communications. The work focuses on the COVID-19 vaccination, but the findings and the recommendations also inform other pandemic health-protective behaviours (e.g., mask-wearing, testing) and other health behaviours more generally (e.g., cancer screening, treatment adherence). We conducted an online study with UK and US respondents in January 2022 (N = 2,433). Participants indicated whether they had received their first, second (together referred to as primo vaccination) and booster vaccinations for Covid and their reasons for these decisions. They also completed a series of questions about trust, socio-psychological characteristics and economic situation.
New and specific barriers to the uptake of the booster dose
The data shows that fewer people had taken the booster vaccine compared to the first round of Covid vaccination and fewer people had a positive attitude towards the COVID-19 booster vaccine. In January 2022, 83% of the respondents had completed their first course of Covid vaccination. That figure dropped to 68% for the booster vaccination (including people who had booked their vaccination). Furthermore, only 74% of the respondents had a positive attitude about the booster, whereas 83% had a positive attitude towards the first course of Covid vaccination - a loss of 9 percentage points in support of the vaccine. This fall in vaccine support shows that there are new and specific barriers to the uptake of the booster dose. The most common reason given by participants for refusing the booster was its lack of effectiveness and the risks of adverse side effects.
Predictors of the booster uptake
Respondents’ knowledge about Covid and about vaccines heavily predicted their vaccination decision. Where their perception that the vaccine was effective, that they had sufficient knowledge, and their perception that COVID-19 was dangerous positively predicted the booster uptake. On the other hand, using social media for vaccine information and believing in conspiracy theories predicted the booster uptake negatively. The tendency to refuse the Covid booster vaccine was also connected with: greater distrust in the healthcare system, a less positive vaccine social norm, and a greater vaccination control preference (wanting to have a say in the vaccination – which vaccine they have, who administers it, where they have it, and when they have it).
Women, people who experienced more financial hardship, belonging to ethnic minority groups, and people with conservative political leaning were less likely to be vaccinated against Covid. Vaccination was a particularly divisive topic based on people’s political preference, with more conservative leaning voters more reluctant to be vaccinated – a trend in both the UK and the US, but especially strong in the US.
Least trusted sources of information used as often as trusted ones
Respondents were aware that information about vaccines shared on social media was not always trustworthy. In contracts, information shared by the WHO or national health services such as the NHS and the CDC or health practitioners was well trusted. But the sources of information people used did not follow the same patterns: people were almost as often exposed to information about vaccines from social media and from friends and family as health practitioners.
Vaccination differences across racial/ethnic groups
Within our American respondents, people from ethnic minority groups tended to be less vaccinated than the White majority – except for people from Asian backgrounds, who were more likely to be vaccinated. Within UK respondents, we found an important gap in the vaccination rates of ethnic minority groups compared to the White majority for both the primo vaccine and the booster.
Explaining the wide vaccination gap between ethnic minority groups and the majority in the UK
Ethnic minority groups show a strong motivation to protect themselves from Covid. Even though there is a gap in vaccination rates, our data shows that this is not because ethnic minority groups show a weaker motivation to protect themselves against Covid. In our studies, people from ethnic minority groups were more motivated than the White majority to protect themselves against Covid by wearing a facemask than the ethnic majority.
Distrust, vaccination control preference and a lack of inclusive vaccine communication explain the lower vaccination uptake in ethnic minority groups in the UK. The vaccination gap between the ethnic minority groups and the majority in the UK was explained by: a perception that vaccine communication was not inclusive enough; a higher distrust in the healthcare system; a greater vaccination control preference (wanting to have a say on the vaccination process); and a more negative social norm (the perception that fewer people in your community are vaccinated).
We also noted a lack of awareness that people from ethnic minority groups are at higher risk from COVID-19. For various reasons, people from ethnic minority groups in the UK and the US are more likely to contract COVID-19, suffer severe symptoms, and die of COVID-19.(1) Only half of the participants recognised that to be the case, whereas 98% recognised that older people are at higher risk.
Current text vaccination invitations are deemed untrustworthy but changing the message source and the message content improves trust and booking intention
Qualitative data indicate that people judged vaccination invitation text messages as untrustworthy. Participants reported that NHS text messages looked like spam or phishing attempts and were unlikely to use them to book their vaccination appointments. Participants were especially suspicious of the web link presented in the text messages. We tested 15 improved text messages where we systematically varied the source of the message and its content. We found that text messages sent by local GPs/physicians foster more trust and booking intention than messages sent by the NHS vaccine services in the UK or by CVS in the US. We also find that messages including information about vaccine benefits and risks improve trust and booking intention.
Research overview
The recovery from the COVID-19 pandemic cannot start until the pandemic is under control and the most vulnerable are protected. Whilst herd immunity seems in sight, vaccination uptake is variable across countries – and within each country, it varies across groups. The infectiousness level of the COVID-19 disease and the pace at which it mutates mean that virus control strategies need to be applied worldwide.
The World Health Organization is very clear: “No one is safe until everyone is safe”.(2)
Our goal is to better understand variation in vaccination acceptance in the UK and the US, two countries with abundant vaccine supplies. In these countries, people’s vaccination acceptance or refusal is not caused solely by a lack of availability – as may have been the case earlier in the pandemic or is still the case in many other countries.
In this project, we investigate the uptake of the Covid booster vaccine in the UK and the US, and assess factors that explain the booster uptake.
Our research aims to accomplish two main goals:
- To assess the Covid booster vaccination uptake and the factors shaping this uptake.
- To experimentally test text message invitation to foster trust and increase vaccination booking intention.
We conducted an online survey in the UK and the US with 2,342 respondents. The data collection took place in January 2022, when the epidemic situation worsened, first in the UK and then in the US because of the arrival of the Omicron variant, as shown in Figure 1. The samples were similar to the general population in terms of age (18 to 95, mean age: 42, standard deviation = 16) and gender (50% split) and diverse in terms of ethnicity. In the UK sample 14-15% of the participants belonged to ethnic minority groups, as did 30-36% of the US sample, which is close to the makeup of the general population in those two countries.
Figure 1. New cases in the UK and the US in early 2022 when the two surveys were conducted
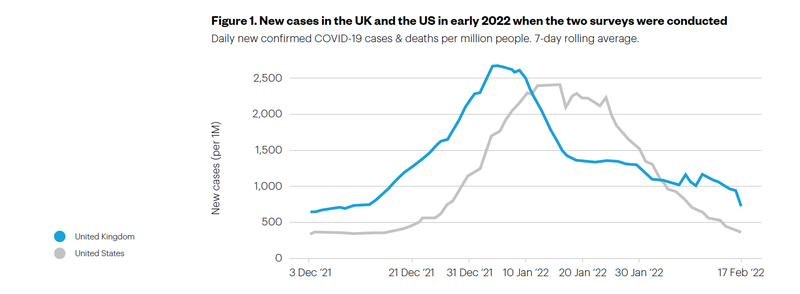
The survey included questions about the vaccination and socio-psychological and economic variables expected to predict vaccination. It included an experimental part assessing the effect of different vaccine invitation text messages on trust perception and booking intention.
The survey included measures of the four pathways hypothesised to explain differences in vaccination uptake between the ethnic minority groups and the majority:
- Distrust in the healthcare system (the extent to which people believe that the healthcare system acted in their best interest).
- Vaccine information inclusiveness (the extent to which people felt vaccination information applied to them, people like them).
- Vaccination control preference (the extent to which people want to have control over which vaccine to get, where, and by whom).
- Vaccination subjective social norm (the proportion of people similar to you who are vaccinated).
The survey included several control measures, including participants’ perceptions of vaccines (risk and benefits), Covid risk and severity, their subjective level of knowledge about the Covid vaccine and conspiracy theory beliefs. Participants reported on the quality of their experience with Covid vaccination and if they had any side effects. Participants also answered questions about their health (e.g., history of Covid infection), their socio-economic status (e.g., income, subjective social status, any experience of financial hardship) and political orientation (party and conservatism/liberal political tendencies).
Policy opportunities and supporting evidence
Policy opportunities to increase vaccination uptake
Strategies to increase vaccination uptake
- Educate: Inform people about the safety and effectiveness of the COVID-19 booster. Debunk misinformation about vaccine risk and benefits wherever possible
- Bridge the political divide regarding vaccination: We recommend that political leaders from different parties promote vaccination together with health experts who are judged more trustworthy (e.g., “The Covid vaccine is safe and effective. The WHO is clear on this matter and strongly recommend that we all get vaccinated when our turn comes”)
- Reach out to a diverse audience on social media: Continue to share health information via social media. Although they are not trusted sources, they are actually often used. This will be especially useful for people from ethnic minority groups who tend to trust more information from social media
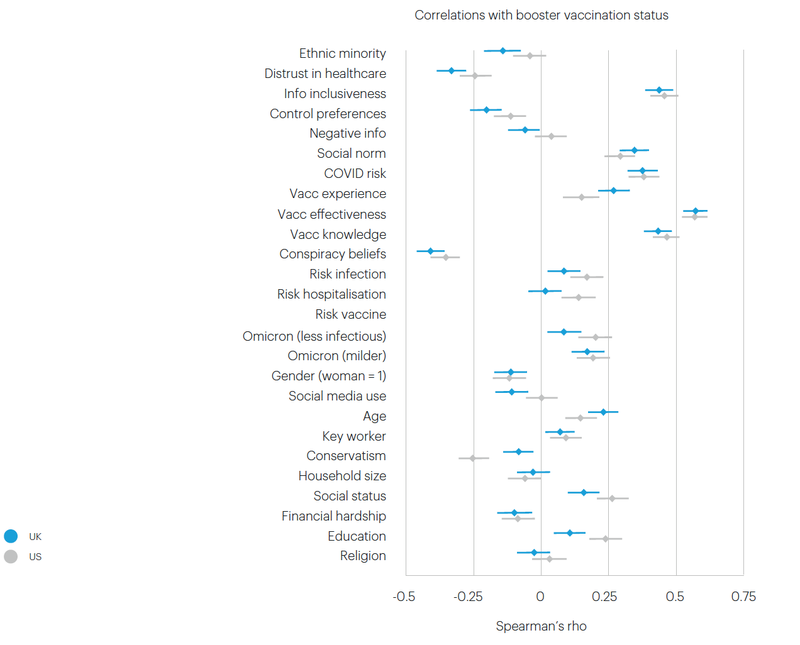
Our survey data (N = 2,342) reveal that respondents’ knowledge about Covid and about vaccines heavily predicted their vaccination decision. Their perception that the vaccine was effective, they had sufficient knowledge, and that COVID-19 is dangerous each positively predicted the booster uptake. On the other hand, using social media for vaccine information and believing in conspiracy theories predicted the booster uptake negatively.
The tendency to refuse the Covid booster vaccine was also connected with greater distrust in the healthcare system, a less positive vaccine social norm, and a greater vaccination control preference (wanting to have a say in the vaccination – which vaccine, done by who, where, when).
Women, people who experienced more financial hardship, those who belonged to ethnic minority groups, and people with conservative political leaning were less likely to be vaccinated against Covid. The data shows that vaccination was a particularly divisive topic based on people’s political preference, with conservative voters more reluctant to be vaccinated – a trend in both the UK and the US, but especially strong in the US.
People from the US were less likely to be vaccinated than people in the UK, a tendency consistent with national-level reports on vaccination.4 Compared to British respondents, American respondents reported a greater distrust in the American healthcare system, greater control preference, more exposure to negative information about vaccines, greater beliefs in conspiracy theories and greater use of social media. The US results highlighted the importance of a national, trusted healthcare services provider, like the NHS.
Figure 2. Predictors of the COVID-19 booster uptake in the UK (blue) and the US (grey)
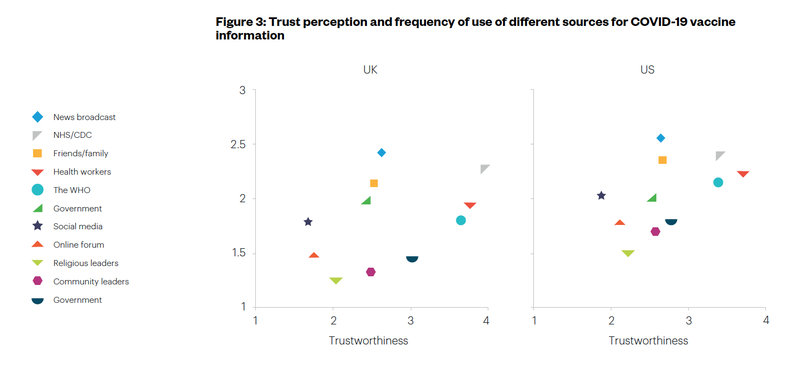
Overall, respondents trusted experts more for information about the Covid vaccine. As shown in Figure 3, the WHO, the NHS/CDC, and health workers were the top three most trusted sources (as shown on the right-hand side in the plot), whereas social media, online forums and religious leaders were the three least trusted sources.
Interestingly, the frequency of use of these sources did not follow the same pattern as the perceived trustworthiness. Participants judged health experts more trustworthy, but they tended to find more information about vaccines on social media or via family and friends.
Figure 3. Trust perception and frequency of use of different sources for COVID-19 vaccine information
To increase vaccination uptake in ethnic minority groups
- Raise awareness that ethnic minority groups are at higher risk from COVID-19. Inform people that people from ethnic minority groups in the UK and the US are at higher risk from COVID-19. Provide a clear breakdown about the risk of infection and the risk of hospitalisation as well as the risk of death
- Provide vaccination control. For example, give people the opportunity to select which vaccine they can get, who will deliver the vaccine or where it will take place. Highlight how being vaccinated provides people more control over their life as it reduces their risks of infection and their risk of infecting others (e.g., “Take back control and get your booster today”)
- Provide autonomy supportive messaging. Use health messaging that empowers people to make decisions, offering them the autonomy and the freedom to choose. This will be especially helpful for people from ethnic minority group
- Provide more inclusive health communication. Public health authorities should share vaccine data, regarding effectiveness and risks broken down per group of interest, so that people are aware that the information shared applies to them. This will be especially useful for people from ethnic minority groups since they are not convinced that vaccine risk and safety apply to them/people like them
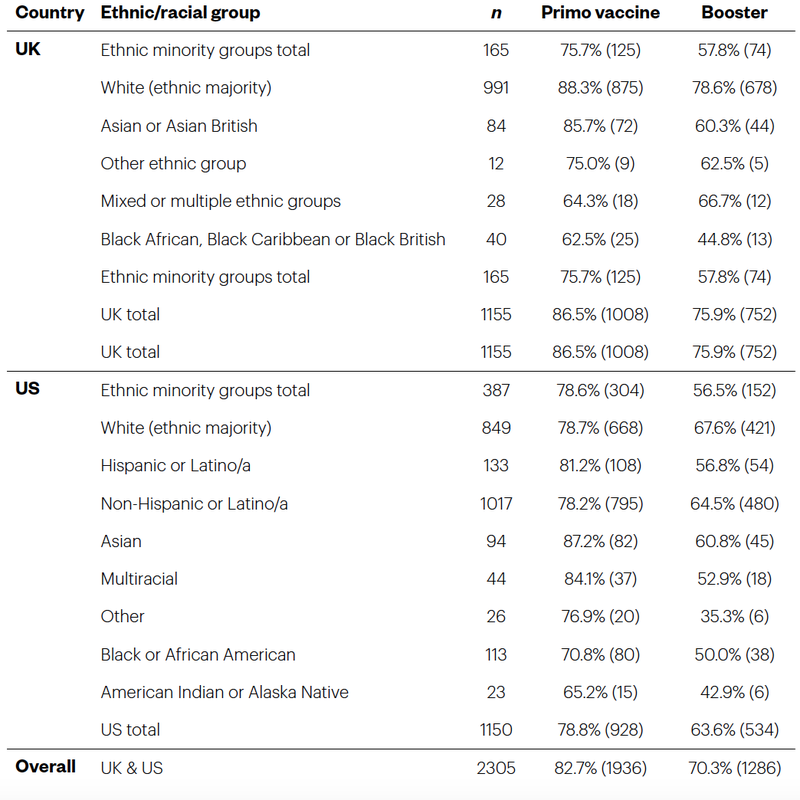
We found important differences in Covid vaccination uptake across ethnic groups. In the US, we found that the ethnic minority groups were as vaccinated as people from the White majority, but this is because people from the Asian minority were more vaccinated than people from other ethnic minority groups, where vaccination levels were lower than in the White majority. In the UK, the vaccination rates in ethnic minority groups were consistently lower than that of the White majority. We note some differences in willingness to be vaccinated, particularly in the Asian/ Asian British and Black/Black British populations, confirming existing inequalities recognised by the NHS regarding COVID-19 and other vaccines.(5)
Our data suggest that the lower uptake of vaccination does not necessarily stem from a reluctance of people from ethnic minority groups to protect themselves or to follow government guidelines. In fact, the data show that they are more motivated than the White majority to protect themselves against COVID-19. Our data show that people from ethnic minority groups were, on average, more likely than the majority to wear facemasks. Wearing a mask is an important health-protective behaviour that affords users a sense of control.
Only half of the participants believed that people from ethnic minorities in their country of residence were more at risk from Covid. Our data show that only half of the participants recognised that to be the case, whereas 98% recognised that older people are at higher risk. Consistent with this, people from ethnic minority groups felt they were equally likely to contract the COVID-19 virus as people from the majority, despite being more likely to do so, but they recognised that they were more likely to suffer severe symptoms. This finding clearly shows a lack of public health communication and education on this point.
Table 1. People from ethnic minority groups were globally less likely to be vaccinated against COVID-19.
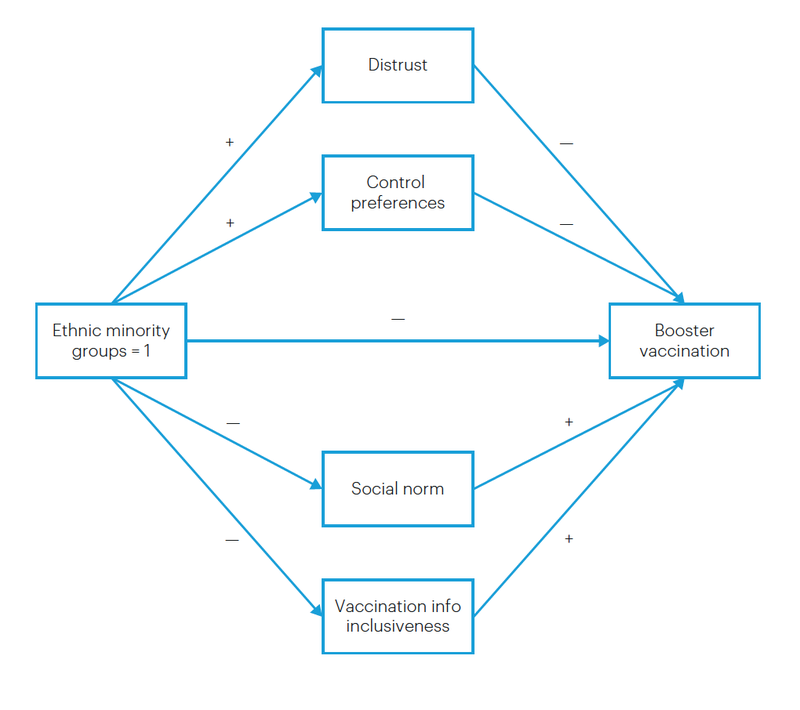
As shown in Figure 4, distrust in the healthcare system, vaccination control preference, and a lack of inclusive vaccine communication explain the lower vaccination uptake in ethnic minority groups in the UK. The difference in vaccination rates between ethnic minority groups and the ethnic majority was explained by higher levels of distrust in the healthcare system and greater vaccination control preferences – which predicted vaccination negatively. People from ethnic minority groups also felt that vaccination communication was not inclusive (e.g., the evidence about effectiveness did not apply to them) and were aware of a lower social norm (the belief that people within your social group are less likely to be vaccinated). Both of those factors were positive predictors of vaccination uptake.
Figure 4.
Policy opportunities to foster trust in vaccination and increase appointment booking
To foster trust in vaccination and increase appointment booking
- Use trustworthy message senders such as GP/family physicians
- Focus on vaccine benefits and risks
- Use vaccination booking web links that are easy to read and identify a clear and trusted website host
Participants in an online qualitative survey reported that the text messages felt like scams, partly because of their web links. Most comments were quite negative, as
people believed that the text looked suspicious. For example. respondents made the
following comments:
Standard information but lacking a secure link and with a third party, so not trustworthy enough to click and follow link.
UK Male, aged 40-49 years
The links sent in the messages are from third party websites and not from the NHS.
UK Female, aged 20-29 years
The text was coming from a third party so I wasn’t sure if I should trust it.
US Female, aged 30-39 years
I would not click the link as it has a third party email address.
UK female, aged 40-49 years
We designed alternative messages sent by different sources and tested if recipients would find them more trustworthy and would be more likely to book their vaccination appointment via the link in the text message. In two studies (N = 1,143 and N = 1,199), four groups of participants judged four different text message invitations to have the Covid booster vaccine. The text messages varied in sources and content, as shown in the experimental flow in Figure 5. The results show that invitation text messages including information about the vaccine benefits and risks elicited more trust and an increased likelihood to book. Changing who sent the message led to increments in trust and booking intention, especially in the US, where a pharmacy chain was the control condition – but also in the UK, in comparison to the NHS.
Figure 5.

Figure 6.
Concluding comment
The WHO Covid pandemic motto “This pandemic is not over anywhere until it is over everywhere.” (6) highlights the need to address health inequalities across countries and groups within countries, which we have tried to do in this work. However, the motto also raises the question of the equity of vaccine distribution across countries, especially their distribution in lower-income countries. Whilst high-income countries are distributing boosters to their populations, many countries cannot provide the first dose to the most clinically vulnerable. The wide distribution of the third dose in high-income countries reduces a lifesaving supply to other countries, and the high demand keeps the prices of vaccines high. Sharing patents would be an obvious solution that would save countless lives. A fairer, global, coordinated approach to the distribution of the vaccine is essential. High-income countries cannot separate themselves from the rest of the world if they wish to effectively combat this pandemic.
References
Collaborative, The OpenSAFELY. “Ethnic Differences in COVID-19 Infection, Hospitalisation, and Mortality: An Opensafely Analysis of 17 Million Adults in England.” Lancet (London, England) 397, no. 10286 (2021): 1711.
Feldman, Justin M., and Mary T. Bassett. “Variation in COVID-19 Mortality in the Us by Race and Ethnicity and Educational Attainment.” JAMA Network Open 4, no. 11 (2021): e2135967-e67. https://doi.org/10.1001/ jamanetworkopen.2021.35967. https://doi.org/10.1001/jamanetworkopen.2021.35967.
Loomba, Sahil, Alexandre de Figueiredo, Simon J. Piatek, Kristen de Graaf, and Heidi J. Larson. “Measuring the Impact of Covid-19 Vaccine Misinformation on Vaccination Intent in the Uk and USA.” Nature Human Behaviour 5, no. 3 (2021/03/01 2021): 337-48. https://doi.org/10.1038/s41562-021-01056-1. https://doi.org/10.1038/s41562021-01056-1.
Mayo Clinic. “U.S. COVID-19 Vaccine Tracker.” 2022. https://www.mayoclinic.org/coronavirus-covid-19/vaccine- tracker.
NHS. Vaccination: Race and Religion/Belief. (2021). https://www.england.nhs.uk/south-east/wp-content/ uploads/sites/45/2021/05/Vaccination-and-race-religion-and-belief-A4.pdf.
“Coronavirus (COVID-19) Cases.” 2022, https://ourworldindata.org/covid-cases.
Pinheiro, Paulo S, Heidy N Medina, Zelde Espinel, Erin N Kobetz, and James M Shultz. “New Insights into the Burden of COVID-19 Mortality for Us Hispanics and Blacks When Examined by Country/Region of Origin: An Observational Study.” The Lancet Regional Health-Americas 5 (2022): 100090.
UK Health Security Agency. “Coronavirus (COVID-19) in the Uk Dashboard: Vaccinations.” 2022https://coronavirus.data.gov.uk/details/vaccinations.
WHO. “Vaccine Equity.” 2021. https://www.who.int/campaigns/vaccine-equity.
“No One Is Safe from COVID-19 until Everyone Is Safe.”, 2021, https://www.who.int/news-room/photo-story/ photo-story-detail/No-one-is-safe-from-COVID19-until-everyone-is-safe.
Citations
1 Paulo S Pinheiro et al., "New insights into the burden of COVID-19 mortality for US Hispanics and Blacks when examined by country/ region of origin: An observational study," The Lancet Regional Health-Americas 5 (2022); Justin M. Feldman and Marl. Bassett, "Variation in COVID-19 Mortality in the US by Race and Ethnicity and Educational Attainment," JAMA Network Open 4, no. 11 (2021), https://doi.org/10.1001/jamanetworkopen.2021.35967, https://doi.org/10.1001/jamanetworkopen.2021.35967; The OpenSAFELY Collaborative, "Ethnic differences in COVID-19 infection, hospitalisation, and mortality: an OpenSAFELY analysis of 17 million adults in England," Lancet (London, England) 397, no. 10286 (2021).
2 "No one is safe from COVID-19 until everyone is safe.," 2021, https://www.who.int/news-room/photo-story/photo-story-detail/No-one-issafe-from-COVID19-until-everyone-is-safe.
3 "Coronavirus (COVID-19) Cases," 2022, https://ourworldindata.org/covid-cases.
4 Mayo Clinic, "U.S. COVID-19 vaccine tracker," (2022). https://www.mayoclinic.org/coronavirus-covid-19/vaccine-tracker; UK Health Security Agency, "Coronavirus (COVID-19) in the UK Dashboard: Vaccinations," (2022). https://coronavirus.data.gov.uk/details/vaccinations
5 NHS, Vaccination: race and religion/belief (2021), https://www.england.nhs.uk/south-east/wp-content/uploads/sites/45/2021/05/Vaccination-and-race-religion-and-belief-A4.pdf.
6 WHO, “Vaccine Equity,” (2021). https://www.who.int/campaigns/vaccine-equity.
Summary
- Published
© The authors. This is an open access publication licensed under a Creative Commons Attribution-NonCommercial- NoDerivs 4.0 Unported License
To cite this report: British Academy (2022), Bridging the Vaccination Gap: Policy Opportunity, The British Academy, London
- DOI doi.org/10.5871/c19-recovery/M-J-H-S-CO- C-B-W-B-C-M-T-C-M-S-G-V-T-D-H-R-W (Opens in a new window)